Dr. Teoh Mei Shi
Consultant Breast, Endocrine & General Surgeon
MBBS (India), MS (USM), Fellowship Breast Oncoplastic Surgery
 Breast Cancer is the most common cancer amongst women in the world. Incidence of breast cancer is increasing and the lifetime risk of developing breast cancer in Malaysia is one in 15 women. In developed countries, the lifetime risk of developing breast cancer in women is as high as 1 in 8 women. With more awareness and screening for breast cancer, women are detecting breast cancers earlier, which are smaller and have better survival outcome.
Breast Cancer is the most common cancer amongst women in the world. Incidence of breast cancer is increasing and the lifetime risk of developing breast cancer in Malaysia is one in 15 women. In developed countries, the lifetime risk of developing breast cancer in women is as high as 1 in 8 women. With more awareness and screening for breast cancer, women are detecting breast cancers earlier, which are smaller and have better survival outcome.
Treatment for breast cancer has evolved significantly over the last few decades due to better understanding of the tumor biology and its behavior. This has led to better adjuvant therapy like systemic chemotherapy, radiation therapy, hormonal therapy and targeted therapy. For most of the earlier twentieth century, Halsted radical mastectomy was the standaradised operation for all stages of breast cancer resulting in poor cosmetic outcome. However, over the recent decades, breast conserving surgery (BCS) eg. Lumpectomy has become the popular alternative to mastectomy in the treatment of early breast cancer.
When detected early, the breast conserving surgery involves a lumpectomy followed by 4-6 weeks of external beam radiotherapy to the whole breast and boost to the tumor bed. This combined method has been proven to reduce local recurrence of breast cancer by 60-70%. However, the side effects of whole breast radiotherapy treatment can be detrimental eg. pain and oedema to the breast, skin fibrosis, fatigue and tiredness and in some cases, there can be associated radiation- induced lung injury and cardiac morbidity.
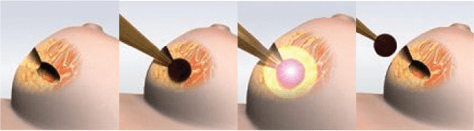
Over the last few years, a new innovative breast cancer therapy known as Intraoperative Radiation therapy (IORT) has become available using the Intrabeam technology. IORT delivers a single dose of radiation directly to the area where the tumor has been removed during surgery.The principle of this approach is to destroy the remaining cancer cells within the lumpectomy cavity where more than 90% of local recurrences usually occur close to the tumor bed.
The Intrabeam IORT is delivered using a miniaturized radiation applicator that is inserted and positioned into the lumpectomy cavity after removal of the tumor. A calculated low energy radiation dose is administered for 20-30mins after which the wound is closed surgically. The operation carries standard risks of bleeding and infection and slightly higher seroma collection comparable to normal breast surgery.
This technology is an excellent option for women having a lumpectomy or breast conserving surgery and is for individuals diagnosed with early-stage breast cancer. The IORT therapy may function as two options ie. as a boost therapy or as a single treatment. Patients are carefully selected and multidisciplinary discussion with breast surgeon and radiation oncologist is carried out to decide the best outcome for the patient.

IORT offers the following advantages:
- Reduced radiation treatment time (single session vs 20-25 sessions) in candidates selected for surgery
- Minimized radiation exposure to surrounding healthy breast tissue, underlying bones, lungs and heart.
- Reduced daily trips to the radiotherapy centre and convenient for those staying very far away.
- Same day radiotherapy treatment and no treatment delay for those going for chemotherapy after surgery
- Provides additional radiotherapy “boost” for high-risk patients who need additional external beam radiation therapy.
The international TARGIT research group has been investigating this new method of delivery radiotherapy for breast cancer after lumpectomy since 1998. The trial compared Intrabeam IORT to standard external beam radiation therapy and found that both treatments were comparable and equally effective with an overall low breast cancer recurrence as well as better breast cancer survival rates. Women who had intraoperative radiotherapy had the advantage of fewer skin side-effects and better cosmetic outcome compared to women who had whole breast external beam radiotherapy.
Conclusion
Intrabeam IORT will be a technology of the future for breast cancer treatment. In properly selected cases, the patients can be offered an alternative option whereby they can receive a shorter dose treatment with lesser side-effects to the breast. It can also be time saving, cost-effective and offers the patient an overall better quality of life.
This treatment will be available at Loh Guan Lye Specialists Centre where a dedicated and trained team of Breast Surgeons and Radiation Oncologists can be consulted to see if you are eligible for the treatment.