Gastroesophageal Reflux Overview
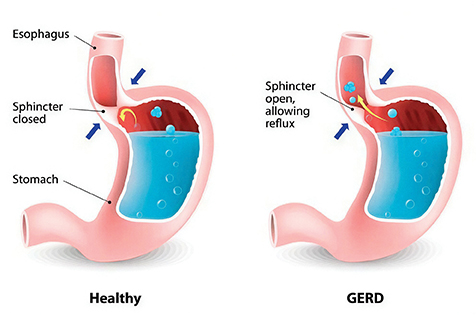
Gastroesophageal reflux, also called acid reflux, occurs when stomach contents back up into the esophagus (food pipe) and/or mouth. Occasional reflux is normal and can happen in healthy people, most often after eating a large meal. Most episodes are brief and do not cause bothersome symptoms or complications. In contrast, people with gastroesophageal reflux disease (GERD) experience bothersome symptoms or damage to the esophagus as a result of acid reflux.
GERD Risk Factors
Certain factors increase a person’s risk of developing GERD, including:
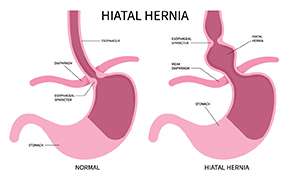
• Hiatal Hernia — This occurs when part of the upper stomach pushes through the diaphragm into the chest. The diaphragm has an opening for the esophagus to pass through, which enlarges in people with a hiatal hernia, allowing the stomach to move upward. This shift increases acid reflux because the lower esophageal sphincter (the valve at the base of the esophagus) becomes less tight.
• Obesity — People who are obese or overweight have an increased risk of GERD and hiatal hernia. While the reasons for this are not completely understood, it is partly related to increased pressure in the abdomen.
• Lifestyle factors and medications — Certain foods (including fatty foods, chocolate, and peppermint), caffeine, alcohol, and cigarette smoking can all worsen acid reflux and GERD. Some medications may also increase the risk.
GERD Symptoms
The most common symptoms of GERD are:
• Heartburn — A burning sensation in the centre of the chest, which sometimes spreads to the throat. It most often happens after a large meal.
• Regurgitation — When stomach contents (acid mixed with bits of undigested food) flow back into your mouth or throat.
Other possible symptoms include:
• Stomach pain (upper abdominal pain)
• Chest pain
• Laryngitis or hoarseness (due to acid irritating the vocal cords)
• Sore throat or cough
• A sensation of a lump in the throat (called globus sensation)
• Nausea and/or vomiting
When to Seek Help
The following signs and symptoms may indicate a more serious problem (also known as alarm symptoms). Tell your healthcare provider right away if you:
• Have difficulty or pain when swallowing (e.g., feeling like food gets stuck in your throat)
• Have no appetite or lose weight without trying
• Experience severe chest pain
• Feel like you are choking
• Notice signs of gastrointestinal bleeding, such as blood in vomit, dark-coloured vomit that looks like coffee grounds, or black tarry stools
• Have persistent vomiting
• Experience any of the above symptoms and are over 60 years old
GERD Diagnosis
If you have the classic symptoms of GERD (heartburn and/or regurgitation), your healthcare provider may diagnose you based on symptoms alone. In such cases, they will likely recommend a trial of medication; if your symptoms improve, it is likely that GERD is the cause.
Additional testing may be needed if you:
• Do not improve after taking a proton pump inhibitor (PPI)
• Do not have the classic symptoms of GERD (heartburn or regurgitation)
• Have alarming symptoms
• Have symptoms that suggest another problem
• Have risk factors for complications such as Barrett’s esophagus or esophageal cancer
It is important to rule out life-threatening problems that can mimic GERD, such as heart disease, which can also cause chest pain and should be evaluated immediately.
If serious conditions are excluded and GERD remains uncertain, your provider may recommend one or more of the following tests:
Upper Endoscopy
An upper endoscopy allows the doctor to directly examine the upper gastrointestinal (GI) tract. A small, flexible tube is passed through the mouth into the esophagus, stomach, and small intestine. The tube has a light and camera that display magnified images on a monitor.
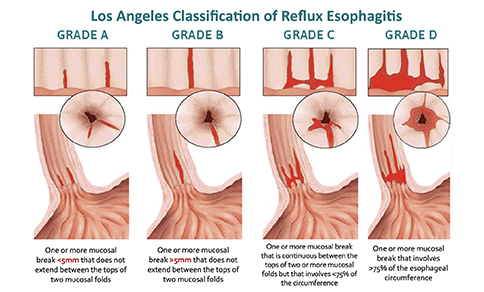
With severe reflux, ulceration or inflammation of the esophageal lining (esophagitis) may be seen. Tissue samples (biopsies) can be taken to evaluate the extent of damage.
Esophageal Manometry
Esophageal manometry measures muscle pressure and movement in the esophagus using a thin tube inserted through the nose. This test checks if the esophagus and lower esophageal sphincter are functioning normally. It may be performed when endoscopy results are normal but symptoms such as chest pain or swallowing difficulty persist.
Esophageal pH Study
An esophageal pH study directly measures acid levels in the esophagus. A thin tube with a sensor is inserted through the nose and left in place for 24 hours. The recorded data helps doctors assess reflux severity and symptom correlation. This test confirms GERD when symptoms exist without visible signs on endoscopy and can also monitor treatment effectiveness.
GERD Complications
Most people with GERD will not develop serious complications, especially with proper treatment. However, severe or long-standing GERD can lead to:
• Erosive esophagitis — Damage to the esophageal lining caused by prolonged acid exposure, which can lead to ulcers or bleeding.
• Esophageal stricture — Scarring and narrowing of the esophagus, causing food or pills to get stuck.
• Barrett’s Esophagus — A condition where the normal squamous cells lining the lower esophagus are replaced by intestinal-type cells due to chronic acid exposure. Barrett’s esophagus slightly increases the risk of esophageal cancer, so regular endoscopic monitoring is recommended.
• Lung and throat problems — Acid reflux into the throat can cause hoarseness, sore throat, or even pneumonia and asthma-like symptoms. Chronic acid exposure may cause lasting lung damage.
• Dental problems — Repeated acid reflux can erode tooth enamel over time.
GERD Treatment
Managing GERD involves both lifestyle changes and medications.
Lifestyle Modifications
• Maintain a healthy weight – Losing excess weight can help reduce reflux.
• Elevate your head during sleep – Raise the head of your bed to prevent acid from flowing upward.
• Sleep on your left side – This position helps keep stomach acid away from the esophagus.
• Eat wisely – Avoid trigger foods such as spicy foods, caffeine, alcohol, peppermint, and fatty meals.
• Quit smoking – Smoking lowers esophageal sphincter pressure and worsens reflux.
• Avoid late meals – Eat smaller, earlier meals and avoid eating close to bedtime.
Medications
• Alginate-containing antacids – These neutralise stomach acid and provide short-term relief in mild GERD. They also form a protective layer that prevents acid from reaching the esophagus.
• Proton Pump Inhibitors (PPIs) – These reduce acid production and promote healing of esophageal inflammation. Examples include dexlansoprazole, lansoprazole, omeprazole, rabeprazole, and pantoprazole. PPIs are typically prescribed for 4–8 weeks and may be continued long-term for complications such as strictures or Barrett’s esophagus.
• Potassium-Competitive Acid Blockers (PCABs) – These newer drugs provide rapid and long-lasting acid suppression and are used in patients who do not respond to PPIs or have severe inflammation or ulcers. Examples include vonoprazan and the recently launched tegoprazan.
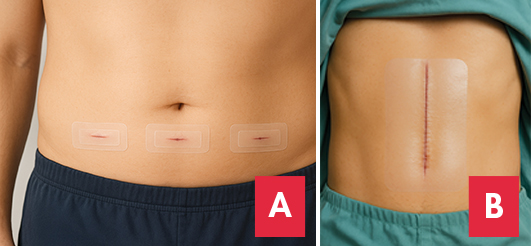
Surgical Treatment
• Lifestyle modifications and medications are very effective in controlling symptoms in most cases. Therefore, surgery is considered only for severe or treatment-resistant (refractory) GERD.
• In general, antireflux surgery involves repairing any hiatal hernia (if present) and strengthening the lower esophageal sphincter.
• The most common surgical procedure is called laparoscopic Nissen fundoplication, which involves wrapping the upper part of the stomach around the lower end of the esophagus to reinforce the valve mechanism.
• However, preoperative manometry and pH studies are essential to confirm the presence and severity of acid reflux and to ensure normal esophageal motility. This helps minimise post-surgical complications such as difficulty swallowing.
Conclusion
GERD is a common condition caused by stomach acid flowing back into the esophagus, leading to symptoms like heartburn and regurgitation. It can usually be managed with lifestyle changes and medications such as alginate-containing antacids, PPIs, or PCABs.
If symptoms are frequent or severe, consult your doctor for proper diagnosis and treatment. Early management not only improves comfort but also prevents complications, helping you live a healthier, more comfortable life.

Dr. Ng Ying Zhuang
Consultant Gastroenterologist, Hepatologist & Physician
MD (FMSMU), MRCP (UK), ESEGH, Fellowship in Gastroenterology & Hepatology (Mal.)
Dr. Ng has extensive clinical experience in the management of gastrointestinal and hepatological diseases, such as gastroesophageal reflux disease, peptic ulcer disease, functional gastrointestinal disorders, inflammatory bowel disease, hepatitis and liver cirrhosis. He performs both diagnostic and therapeutic gastrointestinal endoscopic procedures, including gastroscopy, colonoscopy and endoscopic ultrasound.