“Even though my family is now based in Europe, Malaysia is home for me. I love the warmth, the variety of food and the multitude of cultures, and that’s why I decided to begin my music journey here”
Timur Flores, a prodigious singer-songwriter with a Swiss-Sarawakian heritage, holds a profound connection to Malaysia, where she was born and raised.
Despite her academic achievements, including a Masters degree in Engineering from Oxford University and a stint in the financial industry, Timur made the bold choice to pursue a career in the realm of pop music. Fuelled by her lifelong passion for diverse musical genres and dance, she sought to carve a path for herself in the creative industry.
Blessed with a captivating voice that seamlessly blends melodious tones with an undeniable power, Timur has dedicated recent years to honing her songwriting abilities. Now, she stands resolute in her ambition to establish her presence not only in Malaysia but also on the global stage. Timur, whose very name evokes the spirit of the East, endeavours to channel her songwriting and hip-hop dancing talents back into her homeland, seeking success in the East while captivating audiences worldwide.
Although Timur departed for the UK at the age of 15 to pursue further education, her heart remains firmly rooted in Malaysia. The country’s warm embrace, its vibrant array of culinary delights, and its rich multicultural tapestry serve as a wellspring of inspiration for her musical journey.
Recently, Timur unveiled a tetralogy of songs—Not A Criminal, Sabotage, Love You Now, and Carnival—each accompanied by a meticulously crafted music video. This musical quartet, a testament to Timur’s creativity, weaves an engaging narrative that transcends individual tracks and advocates for championing the innocent against bullying. Collaborating with accomplished teams hailing from LA and Sweden, renowned for their work with notable K-pop groups, Timur’s songs resonate with authenticity and relatability.
Among the multitude of artists who have influenced her, none have left as indelible a mark on Timur as Shakira. Her formative years were filled with admiration for Shakira’s mesmerising dance skills and magnetic stage presence. Now, Timur is poised to release her own self-written song titled “Dance Through My Heart” this summer—a poignant expression of her beliefs and personal experiences.
If you love hide and seek, look for the enchanted Tanao Cafe Bar that is hidden in a historical site in the Phra Nakhon area near the bustling Khao San road in Bangkok, Thailand.
Upon entering the Tanao Cafe Bar, you’ll be greeted by the alluring sight of a grand centennial building owned by the royal family. This building has been renovated to include an indoor, air-conditioned glass dining area. As for those seeking a more al fresco experience, the Tanao Cafe Bar also has a charming garden under the shade of a majestic tree where diners can enjoy their meals while surrounded by a soothing embrace of green nature.
The Tanao Cafe Bar serves the finest food, from home-made pastries to great cocktails.
Prepare to tantalise your taste buds with a selection of signature starters like Miang Bua Luang (Miang Kam wrapped in bite-sized lotus petals), Kratong Tong (Shrimp Salsas in crispy cups), and Somtum Salmon Rolls (Rice paper salmon spring rolls with papaya salad).
Goong Che Nam Pa is a raw prawn dish served with dipping Thai sauce, which is very much a Thai-style sashimi. Moo Pla Ra is fried sun-dried pork served with a spicy-sour sauce that is perfectly complemented by sticky rice and a selection of raw vegetables.
The Tanao Cafe Bar also takes pride in reviving an ancient recipe for Traditional Vermicelli Salad. Rich in flavours of garlic and fried dried shrimp, this salad is a nostalgic journey of flavours through time.
Beside the iconic Khao Ob Saparod (Thai pineapple fried rice with prawns), another must-try signature main dish is the Spaghetti Singha Nua Sua Tai, a captivating fusion of Western and Thai cuisine. In this exquisite creation, al dente spaghetti is paired with spicy Northern Thai sausage.
From classic coffees and teas to an enticing selection of soft drinks, mocktails, cocktails, and more, the drinks menu at Tanao Cafe Bar is carefully crafted to provide a feast for the eyes. It also offers quite a few exclusive dessert creations for sweet lovers, like The Tanao Affogato with Coconut Ice Cream, The Tanao Ruammit, and the Coconut Sundae.
Although Hong Kong reopened its borders in 2023 and launched the “Hello Hong Kong” tourism campaign with 500,000 free flights, the recovery post-pandemic has been slow and challenging. Many shops in popular tourist destinations remain vacant, awaiting new tenants. However, the surviving establishments are grateful to have witnessed a gradual resurgence in business.
Food holds a cherished place in the hearts of Hong Kongers. From local favourites like beef and wonton noodles to succulent roasted meats, the culinary offerings meet a variety of tastes and budgets. Economy rice shops now provide a more diverse range of dishes that are visually appealing; nonetheless, they are commonly served cold. It is a no-go if you are looking for a nice, hot meal. Otherwise, a simple, golden, crispy polo bun coupled with a steaming cup of Hong Kong milk tea is always something to consider.
Many locals grew up with Yung Kee when it first started up as a roadside food stall. Today, the restaurant occupies an iconic building in one of Hong Kong’s most expensive areas, Central District. To visit and savour Yung Kee Restaurant’s famous double charcoal-roasted goose and their other timeless dishes is a must for all tourists. The restaurant features different themed areas for dining, from the nostalgic 1960s Shanghai ambiance to contemporary fusion spaces. For an elevated food experience, it is recommended to make a special booking for private VIP rooms that are available on the higher floors.
Since the return of Hong Kong to China, the Sichuan boiled fish dish (Shui Zhu Yu) has become increasingly popular with the locals. Mian Restaurant, located in the prestigious Murray Hotel, is probably the best around for offering this dish. The fiery delicacy from China combines dried peppers, Sichuan peppercorns, and fresh fish, creating an endorphin rush that is spicy and savoury yet compounded with a numbing experience to challenge the diners senses to “culinary heights’.
The Hong Kong dessert scene is another heaven for food enthusiasts. Crispy egg tarts, egg waffles, steamed milk puddings, and sweet dessert soups are available in almost every corner of the popular spots. While many are queuing outside the Australian Dairy Co. for the famous double steamed milk puddings, it is advisable to opt for Kai Kai, an alternative Michelin-awarded dessert shop that offers equally good steamed milk puddings with shorter queuing times. Speaking of drool-worthy desserts, the amazing artisan cakes of Dan Wen Li by Dominique Ansel are another one not to be missed.
As always, remember to call it a day with a cup of local Hong Kong milk tea or a robust, strong coffee. Immerse yourself in the city’s rich culinary traditions, where old and new intertwine to create a food journey that you will always remember.
A brain tumour is a mass of abnormal cells in the brain. Skull, which encloses the brain, is very rigid. Any growth inside such a restricted space can cause problems.
Brain tumours (BT) can be divided into primary and secondary tumours. Primary BT refers to a tumour that originates from the brain tissue and remain inside the brain. This is further divided into non-cancerous (benign) and cancerous (malignant) tumours.
Secondary brain tumours, also known as a metastatic brain tumour, occurs when cancer cells spread to brain from another organ. Metastatic tumours are considered cancer and are malignant. Secondary brain tumours most often occur in people who have a history of cancer. Rarely, a metastatic brain tumour may be the first sign of cancer that began elsewhere in your body. In adults, secondary brain tumours are far more common than are primary brain tumours.
Any cancer can spread to the brain, but common types include: • Breast cancer • Colon cancer • Kidney cancer • Lung cancer • Melanoma
Data from the Malaysian National Cancer Registry Report (MNCRR) for 2012-2016 revealed a total number of 2,097 cases of brain BT among the Malaysians with 1,117 cases among males and 908 cases females, which ranked as 11th and 13th most common cancer among males and females respectively.
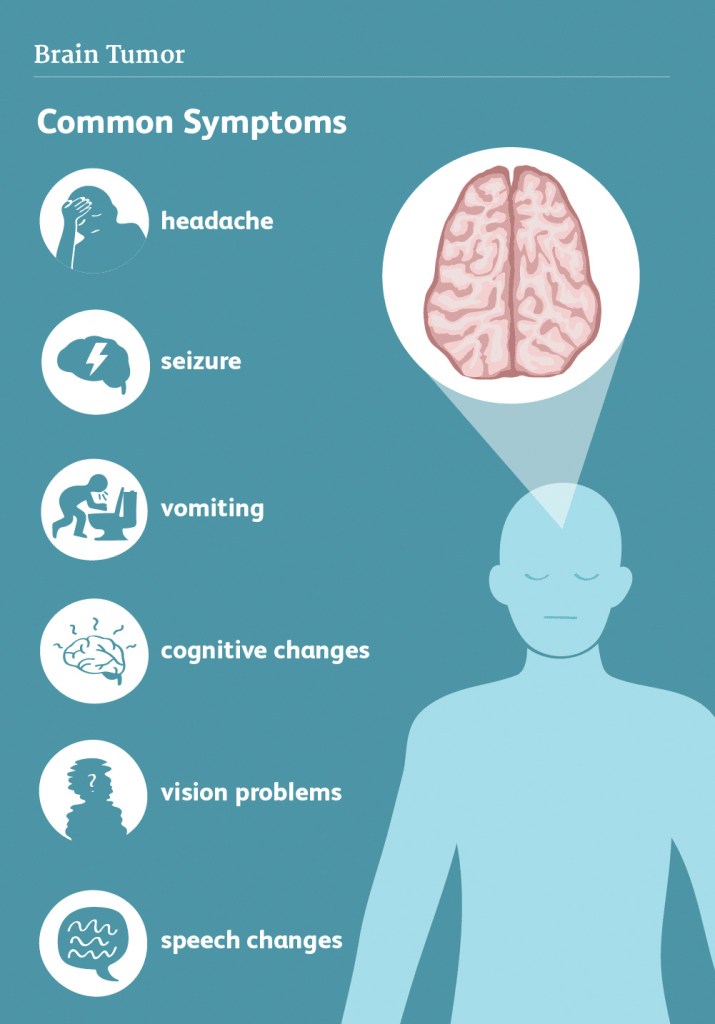
There are many symptoms of brain tumour. The early warning signs of a brain tumour can vary depending on the location of the tumour and the functional system (e.g., motor, sensory, language) it affected. Usually, the specific neurological effects of brain cancer may be associated with the brain tumour’s location or with compression of a certain area of the brain. For instance, a brain tumour near the optic nerve may result in visual problems but potential signs can include weakness, the ability to think, concentrate and balance problems. Individuals with brain tumours may also experience seizures and mental confusion.
But symptoms of brain cancer may not always match up to the tumour location—a brain tumour may cause more compression elsewhere, and the symptoms may correspond to the region of compression, not the area of the cancer.
Any considerably large brain tumour may cause several symptoms because of the pressure produced by the mass. Swelling in the brain caused by the brain tumour or surrounding inflammation may also result in specific symptoms.
Common symptoms of brain tumour may Include: • A headache gets worse over time and certain time of the day • Seizures • Difficulty walking • Numbness in part of the body • Nausea and vomiting • Memory loss • Muscle weakness • Blurring of vision, double vision or vision problems • Difficulty in speaking • Mood and personality changes • Tiredness • Gradual changes in emotional response and intellectual capacity
Some symptoms may be caused by other diseases. The only way to tell for sure is to get tested. Brain cancer may develop overtime, without any obvious signs or with mild symptoms, but it may also suddenly cause severe and fast deterioration.
Imaging tests can help to differentiate if the tumour is a primary brain tumour or secondary cancer that has spread to the brain from elsewhere in the body. Imaging tests show pictures of the inside of the body.
Few factors need to consider when choosing a diagnostic test: • Type of tumour • Signs and symptoms • Age and general health • The results of earlier medical tests
With advancement in imaging techniques can pinpoint brain tumours. Diagnostic tools include computed tomography (CT or CAT scan), Positron Emission Tomography (PET scan) and magnetic resonance imaging (MRI).
CT scan using x-ray to takes images of the inside of the body from different angles. A computer software will reconstruct these pictures into a detailed, 3-dimensional image that shows any abnormalities or tumours. A CT scan can help find blood clot inside the brain and accumulation of fluid in the fluid-filled spaces of the brain, called ventricles. Any bone changes in the skull can also be seen on a CT scan. Sometimes, a contrast medium (dye) is given into patient’s vein (intravenous) before the scan to provide better detail on the image.
Positron emission tomography (PET) or PET-CT scan is used at first to find out more about a tumour while a patient is receiving treatment. It may also be used if the tumour comes back after treatment. A PET scan is usually combined with a CT scan, called a PET-CT scan. A small amount of a radioactive substance is injected into the patient’s body. This substance is taken up by tumour cell as they are actively dividing (growing), they absorb more of the radioactive substance. However, the amount of radiation in the substance is too low to be harmful. A scanner then detects this substance to produce images of the inside of the body.
Magnetic resonance imaging (MRI). An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. A special dye called a contrast medium is given into patient’s vein before the scan to create a clearer picture. MRIs create more detailed pictures than CT scans and are the preferred way to diagnose a brain tumour. The MRI may be of the brain, spinal cord, or both, depending on the type of tumour suspected and the likelihood that it will spread in the brain and spinal cord. There are different types of MRI, doctor will helps determine which type of MRI to use.
A functional MRI (fMRI) provides information about the location of specific areas of the brain that are responsible for muscle movement and speech. During the fMRI examination, the patient is asked to perform certain tasks that cause changes in the brain activity and can be seen on the fMRI image. This test is used to help plan surgery in order to avoid damaging the functional parts of the brain while removing the tumour.
Magnetic resonance spectroscopy (MRS) is a test using an MRI that provides information on the chemical composition of the brain. It can help tell the difference between any dead tissue caused by previous radiation treatments and new tumour cells in the brain.
A sample of the tumour’s tissue is the only definitive way a brain tumour can be diagnosed. A sample of tumour tissue for examination under a microscope by a pathologist, a doctor who specialises in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease. A biopsy can be done as part of surgery to remove the entire tumour. Or surgery may be done as a separate procedure if completely removing the tumour is not possible because of its location or a patient’s health.
Treatment for brain tumours depends on the specific size and type of the mass as well as the patient’s specific tolerance for medications. Treatment options include medications to control seizures, surgery and steroid medications, as well as radiation and chemotherapy. Individuals with tumours that have the potential to grow rapidly may benefit from targeted therapy treatments in which specific parts of the cell are treated to hinder their growth.
Dr. Ch’ng Chee How
Neurosurgeon
MB BCh BAO (NUI), M.Surg. (Neurosurgery) (USM), Clinical F’ship in Skullbase & Braintumor (Korea)
Dr. Ch’ng Chee How is a resident Consultant Neurosurgeon with special interests in Brain Tumour and Minimally Invasive Endoscopic Skull Base Surgery.
He has gained vast experience in Brain and Spine Surgery from working at various tertiary neurosurgical centres including Hospital Pulau Pinang, Hospital USM, Hospital Kuala Lumpur, Hospital Sultanah Aminah (Johor) and Hospital Queen Elizabeth (Sabah). In 2018, he was conferred the Excellent Service Award from Hospital Pulau Pinang for exemplary overall performance.
by Dr. Lim Shyang Yee, General, Upper Gastrointestinal & Bariatric Surgeon
Gastro-esophagus junction is where your food pipe (esophagus) joins the stomach. Cancer which starts from the inner lining of this junction is called gastro-esophagus cancer.
It may be sometimes difficult to tell the difference between stomach, esophagus and gastro-esophagus cancer. In combination esophagus and stomach cancer are the 4th most common cancer. Both cancers in combination are the second most cause of cancer deaths in Malaysia. They can behave differently to cancers of the stomach and esophagus.
In Malaysia, the incidence of esophagus cancer located at the gastro-esophagus junction has increased from 55% to nearly 70% over the last 15 years. Yet 70-80% of patients with this cancer present to specialist very late either stage III or IV of the disease.
Who is at risk? • Chronic Gastroesophagus Reflux Disease (with or without Hiatus Hernia) • Obesity: Higher incidence of hiatus hernia and GERD • Barrett’s Esophagus: Pre-cancerous condition. • Smoking & Excessive Alcohol
How do I know? Early cancer does not have a specific symptom. Dyspepsia or indigestion is a non-specific symptom. Most patients have difficulty of swallowing by the time they seek consultation.
Upper endoscopy examination under sedation (inserting a flexible camera inside the esophagus and stomach through the mouth) to visualize any growth and take sample for confirmation of the diagnosis.
Once diagnosis is confirmed, radiology imaging like PET-CT scan to determine the stage of the cancer and doctor to discuss treatment option.
Can this cancer be cured? Stage of cancer determined the curability of the cancer. If pre-cancerous condition like Barrett’s esophagus is detected early on endoscopy, it can be burned with endoscopic radiofrequency ablation (RFA) and prevent progression to cancer.
Early cancer can be treated with endoscopic resection (shaving the inner layer of the gastro-esophagus mucosa/lining).
Advanced stage II and III cancer require pre-operative treatment of chemotherapy before surgical removal of the lower end of esophagus and removal of affected the lymph nodes. If the cancer has spread to significant portion of the stomach, the stomach will require complete removal.
Can I still able to eat after stomach or esophagus resection? After surgical removal of the disease esophagus and small portion of the stomach, the remaining stomach will be used to restore the continuity of the food passage. After recovering from surgery, food must be properly chewed for smooth swallowing.
For cancer that spreads to the stomach and require total removal of the stomach, the small or large intestine (colon) will be used to restore the continuity of the food passage. After recovering from surgery, patient will still be able to eat and consume smaller portion of food with proper chewing and frequent meals. As absorption of food nutrient occur in the small intestine, most patient can live with their regular food and vitamin B12 supplements.
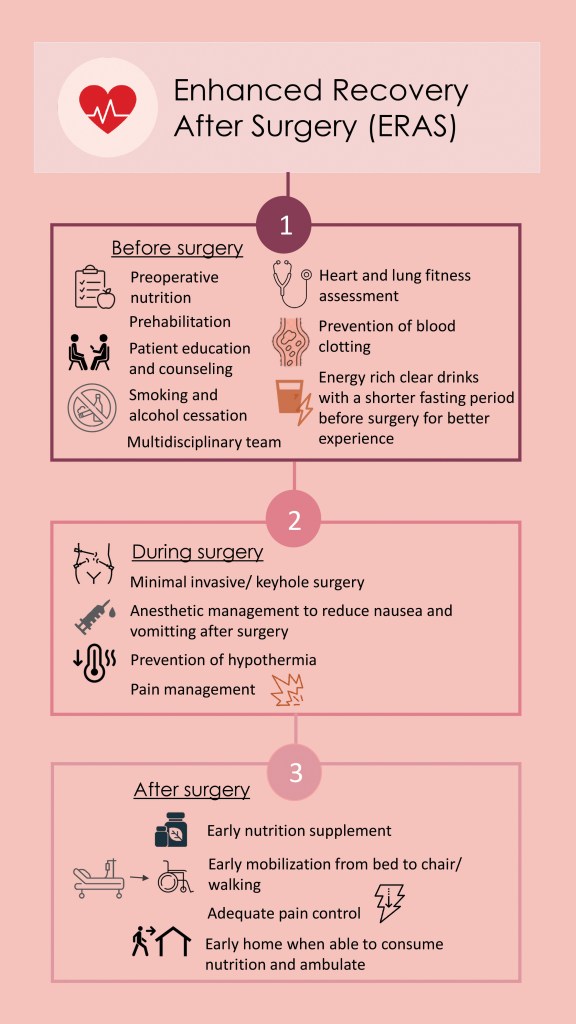
How is the recovery after surgery? Surgery to remove the gastro-esophagus cancer is a major complex surgery. Enhanced recovery after surgery (ERAS) pathway is beneficial for patient who undergoes major complex surgery. Before going for a major sport event athletes undergo proper physical training and adequate preparation & nutrition. Likewise this surgery needs pre-habilitation (activity to improve functional capability and enhanced general wellness before surgery) with adequate pre-surgery nutrition supplements, stop smoking and stabilizing the patient’s co-existing medical conditions before embarking on surgery.
Minimal invasive surgery (keyhole or laparoscopic surgery) can be performed with less post-operative pain and early ambulation.
Is gastro-esophagus cancer preventable? Maintaining a healthy weight, early treatment of GERD and pre-cancerous Barrett’s esophagus can prevent this cancer. Early upper endoscopy is essential for early detection and better survival.
Founded in 1990 in Glashütte, Germany, NOMOS Glashütte has swiftly emerged as a distinguished name in the world of luxury watchmaking. NOMOS Glashütte ‘s dedication to exceptional design and meticulous attention to detail is evident in every watch they create. From the choice of materials to the finishing touches, NOMOS Glashütte ensures that each timepiece is a masterpiece of precision and craftsmanship.
Video source: NOMOS Glashütte
The tetra model from NOMOS Glashütte with a rectangular case and glossy dial are equipped with DUW3001, the highly precise, efficient neomatik movement of the new generation.
Among the four latest tetra watches from NOMOS Glashütte, TETRA NEOMATIK BLUE is no doubt a visually stunning timepiece. It comes with a polished stainless steel case, a dial in deep, glossy blue, complemented by beautifully contrasting hour and minute numerals. The famous hallmarks of Glashütte’s 175 years of watchmaking with the three-quarter plates, ribbing and tempered blue screws can be seen through the sapphire crystal back with limited engraving on the case back.
With a limited edition of 175 pieces worldwide and its remarkable aesthetics, TETRA NEOMATIK BLUE stands as a must-have for watch collectors and watch lovers seeking a unique and exclusive timepiece. Embracing the Feng Shui lucky color of the year for 2023, the deep blue dial adds an extra layer of meaning and significance to this remarkable watch. As the sole available piece in Malaysia, the opportunity to own the TETRA NEOMATIK BLUE becomes even more extraordinary.
“Most people misunderstand, buying gold is not spending; it is an exchange of currency.”
The path to success is one wrought with challenges and red tape for Dato’ Lim Khong Soon, but he is not one to give up. It took him seven years of countless meetings and funds spent, but his perseverance finally paid off when Quantum Metal Sdn Bhd achieved its first milestone of partnering with Bank Muamalat Malaysia Berhad in 2014. Two years later, Quantum Metal officially launched its precious metal trading system solutions. Today, Quantum Metal is one of the largest gold bullion distributors in Malaysia, providing 99.99% premium gold products to the Malaysian market, including government bodies, banks, financial institutions, merchants, and individual dealers.
The idea of setting up a gold profile management company came to Dato’ Lim after a conversation with an Indonesian friend, who told him about the inconvenience of carrying physical gold bars to exchange into US currency.
“I was looking for an alternative business to my electronics recycling business after the government implemented new regulations on the import of waste materials, so the chat with my Indonesian friend inspired me to start Quantum Metal”
Apart from the planning and requirements they have to comply with to set up the company, he said there were also a lot of competitors in the market, and there are still many people who do not understand why investing in gold is a good idea. Instead of giving up, Dato’ Lim saw this as a challenge to overcome.
“To me, business is like boxing matches; the one who stands till the end of the game is the real winner”
Now, Quantum Metal is in 13 countries, including the United States, the United Kingdom, Indonesia, Thailand, the Philippines, and China. The company has about 40,000 consultants and over 400,000 registered members nationwide, with thousands of new members joining daily.
Quantum Metal is introducing a Shariah-compliant gold trading initiative and economic recovery solution to help consumers improve their financial status. The company is also in the process of preparing to be uplisted in Nasdaq after being OTC-listed in the US.
“Today, Quantum Metal has achieved significant milestones over the past ten years, and we are still moving ahead”
It is Dato’ Lim’s wish to incorporate his professional knowledge and experience in gold asset management to educate, lead, and prepare the people to face the fast growing digital economy in metaverse investment. “Most people misunderstand; buying gold is not spending; it is an exchange of currency,” he said.
It is his belief that they must always help others, as per the Scout Oath of “To help other people at all times”. Dato’ Lim says he ensured both his children practises the same values. He has always taught them to be helpful and to help at least one person a day, and that will be their greatest contribution and achievement.
“The ability to use forward-looking statements and future projections in the De-SPAC prospectus allows investors to better gauge a company’s future prospects, hence justifying the higher valuation”
“Listing a company via a SPAC has many advantages: it is less costly, and is a faster and surer way to get listed compared to a traditional IPO”
“SPACs democratised the IPO process”
Datuk Seri Paul Chong is the Managing Partner of Knights Capital Partners, a regional private equity fund, and a Venture Partner at the global investment bank ARC Group. In addition to sponsoring multiple NASDAQ-listed Special Purpose Acquisition Companies (“SPACs”) in 2020-2023, Paul and ARC Group have completed the most NASDAQ SPAC IPOs of any firm in Asia.
He co-founded TNG FinTech Group, Asia’s largest ex-China fintech company with a presence in 16 countries, which owns Tranglo, Malaysia’s largest authorised B2B payments settlement and remittance company.
Paul previously managed the Rothschild Creat Partners Fund (a US$750 million global private equity fund) and the Mitsubishi Creat Fund (a Japan-focused private equity fund worth ¥10 billion/US$130 million).
With three decades of experience in investment banking and private equity, including holding senior positions at Goldman Sachs and UBS Investment Bank, he completed numerous initial public offerings (IPOs) on major exchanges, such as New York, NASDAQ, London, Hong Kong, Australia, Korea, Frankfurt, Singapore, Taiwan, and Kuala Lumpur.
Paul holds a law degree from the London School of Economics and Political Science (LSE) as well as an MBA from the London Business School (LBS). He is also a fellow member of the Institute of Chartered Accountants in England and Wales (ICAEW).
Vice Chairman of the Sports Chiropractic Council Malaysia
“An illness or condition must be viewed holistically in order to provide the best possible care to patients.”
Dr. Taraz-Lee is a multilingual, multicultural graduate of the Anglo-European College of Chiropractic in the United Kingdom.
His own background and interpersonal skills, combined with his diverse educational experience both regionally and abroad, make him a natural communicator who speaks English, Bahasa Melayu, and Mandarin fluently.
Currently the Vice Chairman of the Sports Chiropractic Council Malaysia, Dr. Taraz has extensive first-hand experience with both team and individual sports as an athlete as well as a coach. He strives to help athletes achieve their personal goals and pushes them to perform at their full potential. Alongside this, he dreams of one day representing the country in raising the standards of local sports through sports rehabilitation and performance. He is also a member of the Association of Chiropractic Malaysia.
In terms of work as service, Dr. Taraz finds meaning and purpose in giving back to the community. Having taken part in several service events, one of the most memorable was a trip to India, where a group of chiropractors treated 40,000 people over the course of five days. Dr. Taraz’s perspective on the impact he can have on people’s lives has been shaped by this heart-warming experience.
Dr. Taraz practises integrative medicine and greatly believes that an illness or disease must be viewed in its entirety in order to provide the best possible care to patients.
One of the most common complaints that doctors receive in their daily practice is severe menstrual pain. Most of the time, we may mistake the pain as normal menstrual pain and often endometriosis might be overlooked. Many studies have shown that the diagnosis of endometriosis can be delayed up to 10 to 12 years. The delay in diagnosis of endometriosis could severely affect the fertility of many women while some women develop complications such heavy menstrual bleeding, low blood levels (anaemia), having painful enlarged uterus (adenomyosis) or ovarian endometriotic cysts. At present, there is no objective test to diagnose this disease. Doctors depend on patient’s signs and symptoms to make a clinical diagnosis.
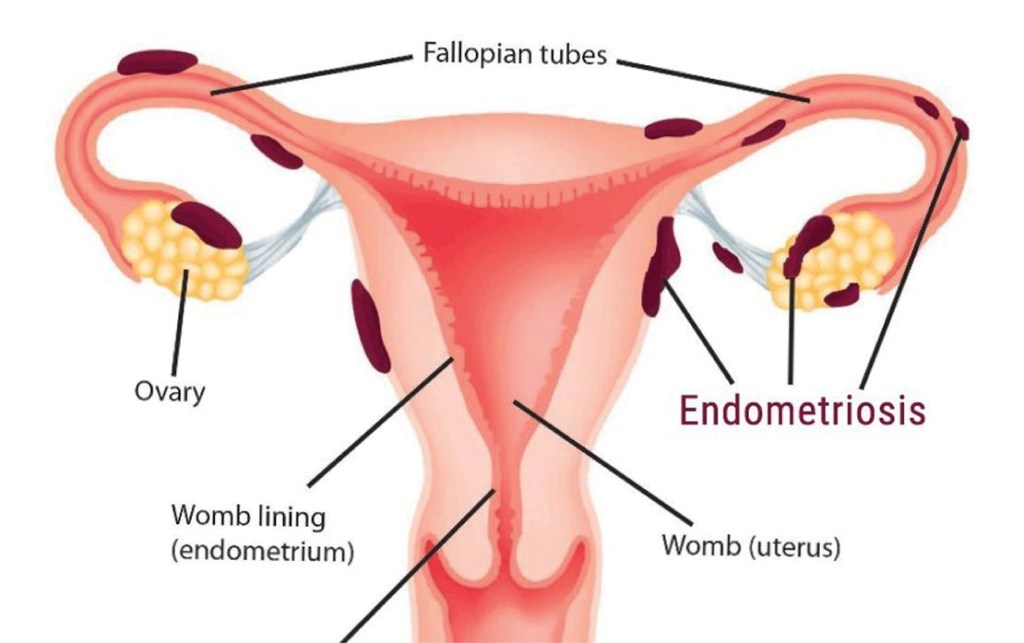
What is endometriosis? Endometriosis is derived from the word “endometrium,” which is the tissue that lines the womb (uterus). Patients with endometriosis have endometrial type of tissue which grows outside of the uterus particularly in the surrounding organs such as bladder, bowels and sometimes, even in the distant parts of the body such as the umbilicus, lungs and the brain.
The endometriotic lesion is influenced by the female hormones. It undergoes proliferation, break downs and bleeds during each menstrual cycle. Its characteristics resemble a normal endometrial tissue which is found inside the womb. With each menses, endometriosis will cause chronic inflammation and the formation of scar tissues inside the pelvis, which can distort the anatomy of the surrounding organs and interfere with their functions.
Endometriosis tissues implant outside the uterus
What causes endometriosis? Doctors and researchers have not identified the cause of endometriosis. One of the most popular and widely believed theory is Sampson’s Theory of Retrograde Menstruation, postulated by Dr. John Sampson in the 1920’s. According to the theory, during each menstrual cycle, a certain amount of menstrual fluid in the uterus is forced into the pelvic cavity via the fallopian tubes. The body usually responds to this kind of spilling by reabsorbing the menstrual fluid back into the circulatory system. However, in some women, due to immune system dysfunction, the fluid is not reabsorbed but instead implants itself and grows on the pelvic and abdominal organs.
We also realise that endometriosis tends to run in families. If your mother or sister has endometriosis, you’re more likely to get it. Research shows that it tends to get worse from one generation to the next.
What are the symptoms and signs of endometriosis?
1. Pelvic pain Most women with endometriosis experience severe pelvic pain, lower back pain and cramps before and during menstruation. The medical term for such severe pain is called dysmenorrhea. Other common complaints include dyspareunia (pain during intercourse), dyschezia (painful defecation) and dysuria (painful urination).
2. Heavy or irregular vaginal bleeding Women with endometriosis may experience excessive menstrual bleeding or bleeding between periods.
3. Infertility Some women with endometriosis may experience little or no pain at all but are unable to conceive and are usually first diagnosed with endometriosis while seeking treatment for infertility. These are usually cases where the formation of scar tissue (adhesions) due to endometriosis, has somehow distorted the reproductive organs and therefore results in inability to conceive.
4. Painful bowel movements Some women may experience bowel pain followed by abdominal bloating, constipation, or diarrhoea. The pain may intensify during menstruation.
Diagnosis There are no specific tests to assess whether a woman has endometriosis. Exploring a patient’s medical history may give the doctor some clue to the presence of this disease, and it is usually accompanied by a pelvic examination.
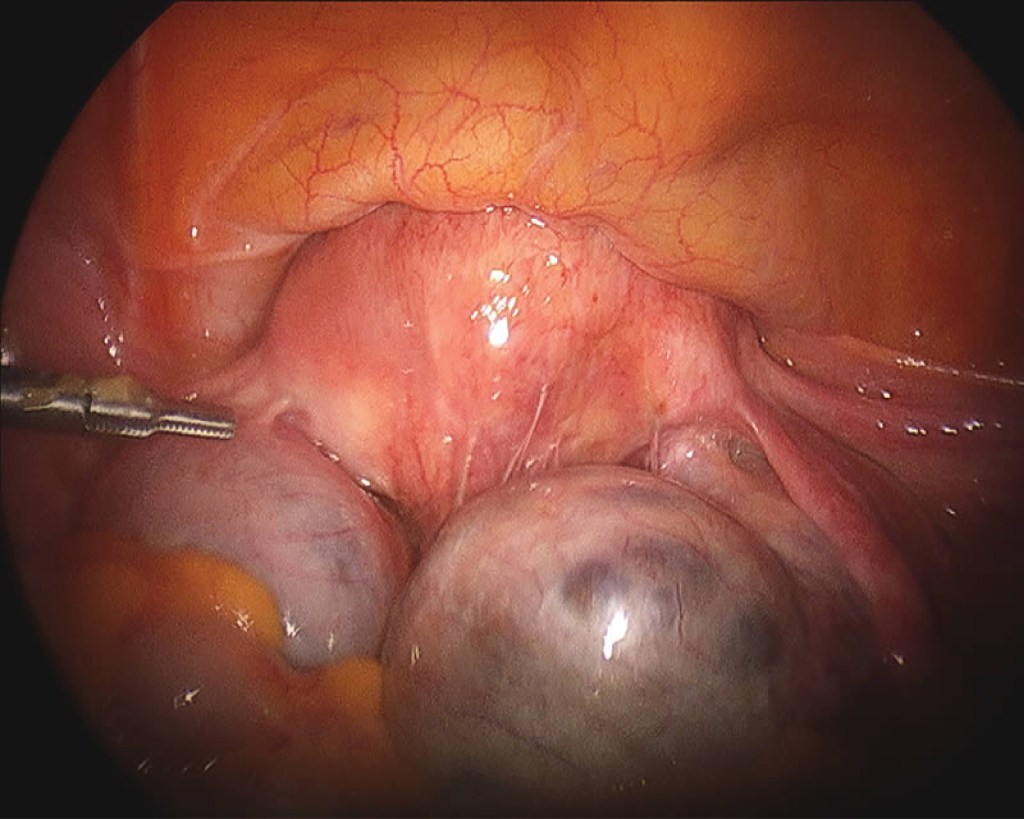
The pelvic examination may reveal irregular painful swellings in the Pouch of Douglas and an enlarged uterus. The pelvic ultrasound may reveal ovarian cysts that appear in the form “kissing cysts” (picture below). Sometimes, the doctor may order a blood test called CA-125 and if it is elevated, it is suggestive of endometriosis.
In some cases, it is possible to be mistaken endometriosis for other gynaecological conditions that have similar symptoms and vice versa. The only reliable way to confirm and verify the suspected diagnosis of endometriosis is through laparoscopy.
Transvaginal ultrasound shows bilateral endometriotic cysts Endometriotic tissues can implant in between uterine muscle walls causing enlarged uterus, heavy menses and severe menstrual pain. The enlarged uterine wall is known as adenomyosis.
Treatment Options There is no cure for endometriosis now and this condition can be difficult to treat. The aim of treatment is to relieve pain, to remove endometriotic tissues to improve fertility and to prevent disease recurrence. Treatment modalities can be divided into 3 categories: a) Pain killers b) Surgery c) Hormonal therapy
a) Pain killers Non-steroidal anti-inflammatory drugs (NSAIDs) are medicines that are widely used to relieve pain, help to reduce inflammation, and bring down a fever; for example, ibuprofen and mefenamic acid. They can be used together in combination with paracetamol for more severe pain. These painkillers are available in pharmacies.
b) Surgery Surgery is the main treatment option for women with endometriosis. Laparoscopic surgery (key hole) is the preferred surgery but sometimes we may need to perform open laparotomy for very complicated cases. The aim of surgery is to diagnose endometriosis as well as to remove as much of the diseased areas as possible.
c) Hormonal therapy Endometriosis is influenced by the hormone oestrogen. Whenever there is menstruation, the endometriotic lesion will grow, causing pain and forming adhesions in the pelvis. By giving hormonal therapy, menstruation is reduced or suppressed and therefore prevents the growth of endometriosis and relieve its symptoms. Hormonal therapies can be given before and essentially after laparoscopic surgery to suppress any remaining tissues. Some of the therapies include:
i. Gonadotropin-releasing hormone (GnRH) agonist ii. Combined oral contraceptive pills iii. Progestogens pills iv. Mirena® (intrauterine device coated with hormone)
Mirena® coil
Can endometriosis recur after surgery? Endometriosis can recur after surgery and medical treatment. The chance of recurrence is higher if endometriotic lesions are not excised completely. If the patient is not contemplating pregnancy immediately after the surgery, continuing medical therapy after surgery to suppress any endometriotic lesion that has not been excised.
Complimentary Therapies Although there is only limited evidence for their effectiveness, some women may find the following therapies helpful to reduce pain and improve their quality of life: • reflexology • transcutaneous electrical nerve stimulation (TENS) • acupuncture • vitamin B1 and magnesium supplements • traditional Chinese medicine • herbal treatments • homeopathy
Is endometriosis associated with ovarian cancer? Studies have shown that patients with ovarian endometriosis have 2-3-fold increased risk of ovarian cancer.
Should pregnancy be recommended as a treatment for endometriosis? Pregnancy might help to reduce endometriosis symptoms only temporarily, but it is not a cure. There are also risks involved, as women with endometriosis are more likely to have pre-term births, increased rates of caesarean sections and an increased risk of miscarriages.
Are there ways to prevent endometriosis? Endometriosis is an idiopathic condition, meaning there is no known cause. There are also no specific ways to prevent endometriosis. However, being aware of the symptoms and whether you could be at higher risk can help you know when to discuss it with a doctor.
Summary Women with endometriosis constantly battle with monthly pelvic pain, and it affects their fertility. Being pregnant with endometriosis may also increase your risk of serious pregnancy complications. Therefore, women should seek consultation with their gynaecologists for an early diagnosis. With early intervention, it may improve their quality of life and reduce severe complications.
Dr. Chua Shih Keat
Obstetrician & Gynaecologist
MD(UPM), MRCOG(UK)
Dr. Chua Shih Keat received his medical degree from Universiti Putra Malaysia and obtained the membership of Royal College of Obstetricians and Gynaecologists (MRCOG), United Kingdom.
Dr. Chua specializes in the care of women during pregnancy and childbirth and in the diagnosis and treatment of diseases of the female reproductive organs. He has been managing women’s health issues for the past 16 years in various health facilities.