by Dr. Lim Shyang Yee, General, Upper Gastrointestinal & Bariatric Surgeon
Gastro-esophagus junction is where your food pipe (esophagus) joins the stomach. Cancer which starts from the inner lining of this junction is called gastro-esophagus cancer.
It may be sometimes difficult to tell the difference between stomach, esophagus and gastro-esophagus cancer. In combination esophagus and stomach cancer are the 4th most common cancer. Both cancers in combination are the second most cause of cancer deaths in Malaysia. They can behave differently to cancers of the stomach and esophagus.
In Malaysia, the incidence of esophagus cancer located at the gastro-esophagus junction has increased from 55% to nearly 70% over the last 15 years. Yet 70-80% of patients with this cancer present to specialist very late either stage III or IV of the disease.
Who is at risk? • Chronic Gastroesophagus Reflux Disease (with or without Hiatus Hernia) • Obesity: Higher incidence of hiatus hernia and GERD • Barrett’s Esophagus: Pre-cancerous condition. • Smoking & Excessive Alcohol
How do I know? Early cancer does not have a specific symptom. Dyspepsia or indigestion is a non-specific symptom. Most patients have difficulty of swallowing by the time they seek consultation.
Upper endoscopy examination under sedation (inserting a flexible camera inside the esophagus and stomach through the mouth) to visualize any growth and take sample for confirmation of the diagnosis.
Once diagnosis is confirmed, radiology imaging like PET-CT scan to determine the stage of the cancer and doctor to discuss treatment option.
Can this cancer be cured? Stage of cancer determined the curability of the cancer. If pre-cancerous condition like Barrett’s esophagus is detected early on endoscopy, it can be burned with endoscopic radiofrequency ablation (RFA) and prevent progression to cancer.
Early cancer can be treated with endoscopic resection (shaving the inner layer of the gastro-esophagus mucosa/lining).
Advanced stage II and III cancer require pre-operative treatment of chemotherapy before surgical removal of the lower end of esophagus and removal of affected the lymph nodes. If the cancer has spread to significant portion of the stomach, the stomach will require complete removal.
Can I still able to eat after stomach or esophagus resection? After surgical removal of the disease esophagus and small portion of the stomach, the remaining stomach will be used to restore the continuity of the food passage. After recovering from surgery, food must be properly chewed for smooth swallowing.
For cancer that spreads to the stomach and require total removal of the stomach, the small or large intestine (colon) will be used to restore the continuity of the food passage. After recovering from surgery, patient will still be able to eat and consume smaller portion of food with proper chewing and frequent meals. As absorption of food nutrient occur in the small intestine, most patient can live with their regular food and vitamin B12 supplements.
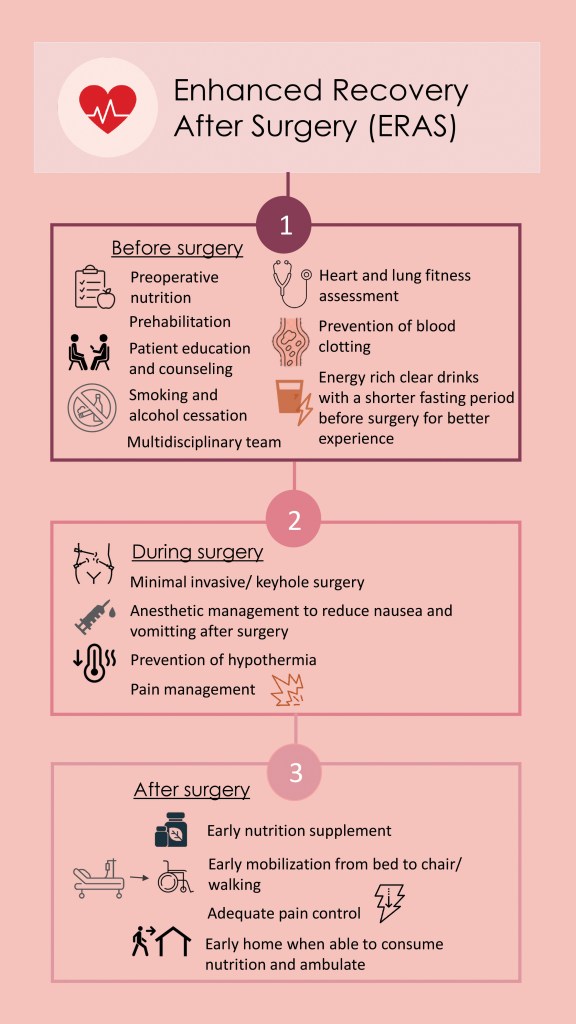
How is the recovery after surgery? Surgery to remove the gastro-esophagus cancer is a major complex surgery. Enhanced recovery after surgery (ERAS) pathway is beneficial for patient who undergoes major complex surgery. Before going for a major sport event athletes undergo proper physical training and adequate preparation & nutrition. Likewise this surgery needs pre-habilitation (activity to improve functional capability and enhanced general wellness before surgery) with adequate pre-surgery nutrition supplements, stop smoking and stabilizing the patient’s co-existing medical conditions before embarking on surgery.
Minimal invasive surgery (keyhole or laparoscopic surgery) can be performed with less post-operative pain and early ambulation.
Is gastro-esophagus cancer preventable? Maintaining a healthy weight, early treatment of GERD and pre-cancerous Barrett’s esophagus can prevent this cancer. Early upper endoscopy is essential for early detection and better survival.
One of the most common complaints that doctors receive in their daily practice is severe menstrual pain. Most of the time, we may mistake the pain as normal menstrual pain and often endometriosis might be overlooked. Many studies have shown that the diagnosis of endometriosis can be delayed up to 10 to 12 years. The delay in diagnosis of endometriosis could severely affect the fertility of many women while some women develop complications such heavy menstrual bleeding, low blood levels (anaemia), having painful enlarged uterus (adenomyosis) or ovarian endometriotic cysts. At present, there is no objective test to diagnose this disease. Doctors depend on patient’s signs and symptoms to make a clinical diagnosis.
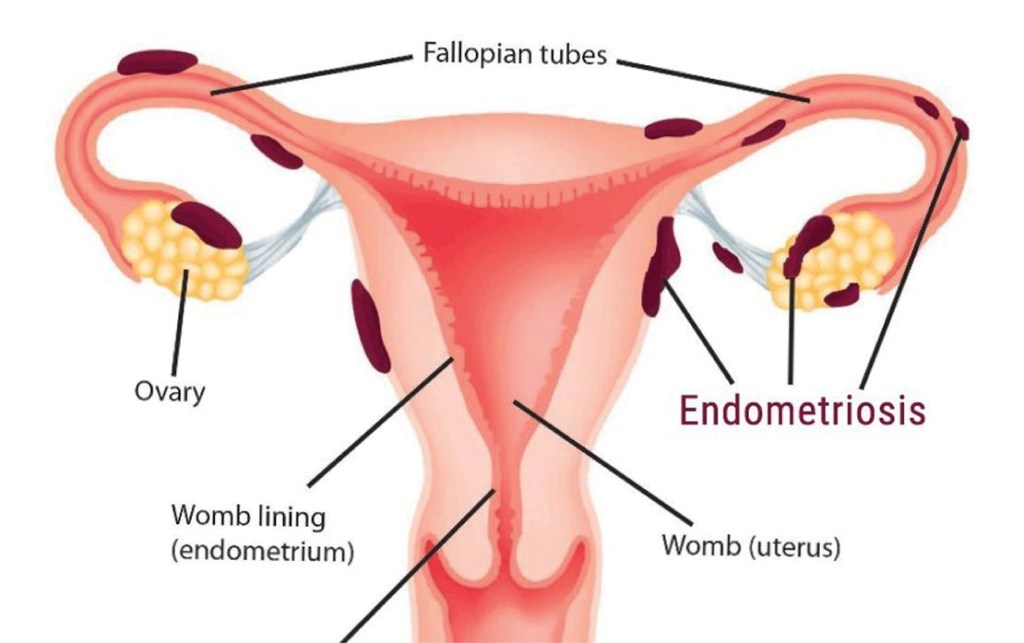
What is endometriosis? Endometriosis is derived from the word “endometrium,” which is the tissue that lines the womb (uterus). Patients with endometriosis have endometrial type of tissue which grows outside of the uterus particularly in the surrounding organs such as bladder, bowels and sometimes, even in the distant parts of the body such as the umbilicus, lungs and the brain.
The endometriotic lesion is influenced by the female hormones. It undergoes proliferation, break downs and bleeds during each menstrual cycle. Its characteristics resemble a normal endometrial tissue which is found inside the womb. With each menses, endometriosis will cause chronic inflammation and the formation of scar tissues inside the pelvis, which can distort the anatomy of the surrounding organs and interfere with their functions.
Endometriosis tissues implant outside the uterus
What causes endometriosis? Doctors and researchers have not identified the cause of endometriosis. One of the most popular and widely believed theory is Sampson’s Theory of Retrograde Menstruation, postulated by Dr. John Sampson in the 1920’s. According to the theory, during each menstrual cycle, a certain amount of menstrual fluid in the uterus is forced into the pelvic cavity via the fallopian tubes. The body usually responds to this kind of spilling by reabsorbing the menstrual fluid back into the circulatory system. However, in some women, due to immune system dysfunction, the fluid is not reabsorbed but instead implants itself and grows on the pelvic and abdominal organs.
We also realise that endometriosis tends to run in families. If your mother or sister has endometriosis, you’re more likely to get it. Research shows that it tends to get worse from one generation to the next.
What are the symptoms and signs of endometriosis?
1. Pelvic pain Most women with endometriosis experience severe pelvic pain, lower back pain and cramps before and during menstruation. The medical term for such severe pain is called dysmenorrhea. Other common complaints include dyspareunia (pain during intercourse), dyschezia (painful defecation) and dysuria (painful urination).
2. Heavy or irregular vaginal bleeding Women with endometriosis may experience excessive menstrual bleeding or bleeding between periods.
3. Infertility Some women with endometriosis may experience little or no pain at all but are unable to conceive and are usually first diagnosed with endometriosis while seeking treatment for infertility. These are usually cases where the formation of scar tissue (adhesions) due to endometriosis, has somehow distorted the reproductive organs and therefore results in inability to conceive.
4. Painful bowel movements Some women may experience bowel pain followed by abdominal bloating, constipation, or diarrhoea. The pain may intensify during menstruation.
Diagnosis There are no specific tests to assess whether a woman has endometriosis. Exploring a patient’s medical history may give the doctor some clue to the presence of this disease, and it is usually accompanied by a pelvic examination.
The pelvic examination may reveal irregular painful swellings in the Pouch of Douglas and an enlarged uterus. The pelvic ultrasound may reveal ovarian cysts that appear in the form “kissing cysts” (picture below). Sometimes, the doctor may order a blood test called CA-125 and if it is elevated, it is suggestive of endometriosis.
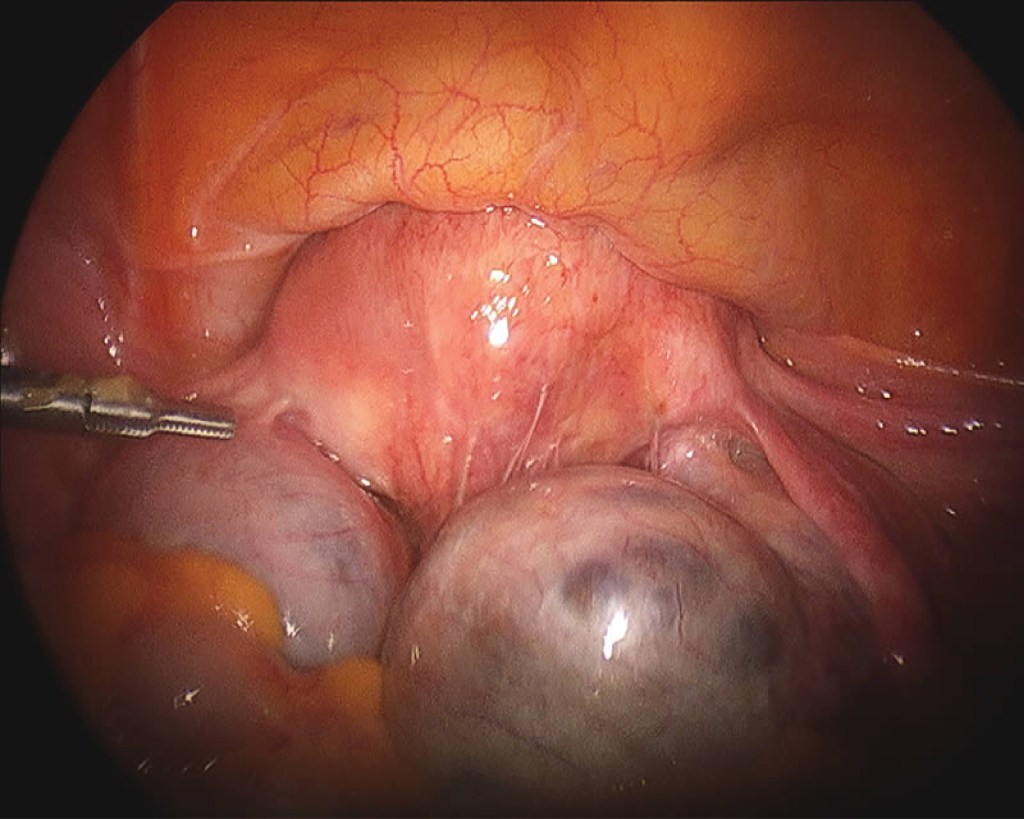
In some cases, it is possible to be mistaken endometriosis for other gynaecological conditions that have similar symptoms and vice versa. The only reliable way to confirm and verify the suspected diagnosis of endometriosis is through laparoscopy.
Transvaginal ultrasound shows bilateral endometriotic cysts Endometriotic tissues can implant in between uterine muscle walls causing enlarged uterus, heavy menses and severe menstrual pain. The enlarged uterine wall is known as adenomyosis.
Treatment Options There is no cure for endometriosis now and this condition can be difficult to treat. The aim of treatment is to relieve pain, to remove endometriotic tissues to improve fertility and to prevent disease recurrence. Treatment modalities can be divided into 3 categories: a) Pain killers b) Surgery c) Hormonal therapy
a) Pain killers Non-steroidal anti-inflammatory drugs (NSAIDs) are medicines that are widely used to relieve pain, help to reduce inflammation, and bring down a fever; for example, ibuprofen and mefenamic acid. They can be used together in combination with paracetamol for more severe pain. These painkillers are available in pharmacies.
b) Surgery Surgery is the main treatment option for women with endometriosis. Laparoscopic surgery (key hole) is the preferred surgery but sometimes we may need to perform open laparotomy for very complicated cases. The aim of surgery is to diagnose endometriosis as well as to remove as much of the diseased areas as possible.
c) Hormonal therapy Endometriosis is influenced by the hormone oestrogen. Whenever there is menstruation, the endometriotic lesion will grow, causing pain and forming adhesions in the pelvis. By giving hormonal therapy, menstruation is reduced or suppressed and therefore prevents the growth of endometriosis and relieve its symptoms. Hormonal therapies can be given before and essentially after laparoscopic surgery to suppress any remaining tissues. Some of the therapies include:
i. Gonadotropin-releasing hormone (GnRH) agonist ii. Combined oral contraceptive pills iii. Progestogens pills iv. Mirena® (intrauterine device coated with hormone)
Mirena® coil
Can endometriosis recur after surgery? Endometriosis can recur after surgery and medical treatment. The chance of recurrence is higher if endometriotic lesions are not excised completely. If the patient is not contemplating pregnancy immediately after the surgery, continuing medical therapy after surgery to suppress any endometriotic lesion that has not been excised.
Complimentary Therapies Although there is only limited evidence for their effectiveness, some women may find the following therapies helpful to reduce pain and improve their quality of life: • reflexology • transcutaneous electrical nerve stimulation (TENS) • acupuncture • vitamin B1 and magnesium supplements • traditional Chinese medicine • herbal treatments • homeopathy
Is endometriosis associated with ovarian cancer? Studies have shown that patients with ovarian endometriosis have 2-3-fold increased risk of ovarian cancer.
Should pregnancy be recommended as a treatment for endometriosis? Pregnancy might help to reduce endometriosis symptoms only temporarily, but it is not a cure. There are also risks involved, as women with endometriosis are more likely to have pre-term births, increased rates of caesarean sections and an increased risk of miscarriages.
Are there ways to prevent endometriosis? Endometriosis is an idiopathic condition, meaning there is no known cause. There are also no specific ways to prevent endometriosis. However, being aware of the symptoms and whether you could be at higher risk can help you know when to discuss it with a doctor.
Summary Women with endometriosis constantly battle with monthly pelvic pain, and it affects their fertility. Being pregnant with endometriosis may also increase your risk of serious pregnancy complications. Therefore, women should seek consultation with their gynaecologists for an early diagnosis. With early intervention, it may improve their quality of life and reduce severe complications.
Dr. Chua Shih Keat
Obstetrician & Gynaecologist
MD(UPM), MRCOG(UK)
Dr. Chua Shih Keat received his medical degree from Universiti Putra Malaysia and obtained the membership of Royal College of Obstetricians and Gynaecologists (MRCOG), United Kingdom.
Dr. Chua specializes in the care of women during pregnancy and childbirth and in the diagnosis and treatment of diseases of the female reproductive organs. He has been managing women’s health issues for the past 16 years in various health facilities.
What is lymphoma? Lymphoma is a cancer of the lymphatic system, which is part of the body’s immune system. The lymphatic system consists of lymph nodes, tonsils, spleen, thymus gland and bone marrow. Lymph fluid contains white blood cells which defend the body against invasion by bacteria, viruses, parasites and other foreign substances. Lymphoma develops when white blood cells called lymphocytes grow out of control.
What are types of lymphoma? There are two major types of lymphomas: Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL), which differ in the way they develop and spread, as well as in the way they are treated. The World Health Organization (WHO) divides HL into two main groups: classical HL (cHL) and nodular lymphocyte-predominant HL (NLPHL). Most patients with HL are diagnosed between 15 and 30 years of age, followed by another peak in adults aged 55 years or older. For NHL, it is a heterogenous group of blood disorder arises from B-lymphocytes, T-lymphocytes, or natural killer (NK) cells. There are more than eighty subtypes of NHL, which can be simplified into two major categories, namely B-cell and T/NK-cell NHL.
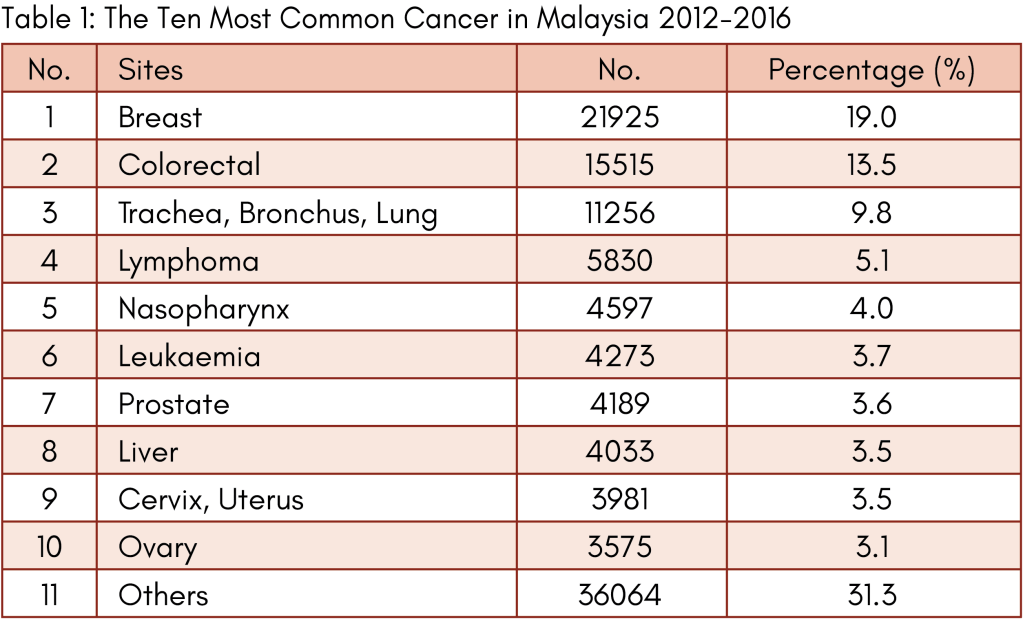
What is the incidence of lymphoma? NHL is more common than HL. Most NHL (85-90%) are from B cells and less than 15% develop from T cells. Classical and nodular lymphocyte predominant HL account for 95% and 5% of all HL respectively. According to Malaysia National Cancer Registry Report 2012-2016, lymphoma is the fourth most common form of cancer overall in Malaysia after breast, colorectal and lung malignancies (table 1).
What causes lymphoma? The causes of lymphoma are not understood. However, people with certain risk factors have a slightly higher chance of developing lymphoma compared with people without these risk factors. Known risk factors for lymphoma include: 1. Immunodeficiency: HIV infection, transplantation, Wiskott-Aldrich syndrome. 2. Infection: human T-cell lymphotropic virus type 1, Epstein-Barr virus, helicobacter pylori. 3. Autoimmune: Crohn’s disease, systemic lupus erythematosus, Sjogren syndrome. 4. Environmental toxins: pesticides, herbicides, certain drugs used to treat cancer.
While siblings and children of patients with lymphoma have a slightly increased risk of developing this disease compared with the general population, there are no clearly identifiable genetic or hereditary factors that can predict this slightly increased risk. Therefore, routine screening for lymphoma among the immediate family members of patients with lymphoma is not recommended.
What are the symptoms? Some patients with lymphoma do not have any obvious signs or symptoms of the disease. The clinical features at presentation reflect a spectrum from low grade to high grade lymphoma. Low grade (also called indolent) lymphomas usually grow slowly, exhibit few symptoms, typically present with widespread disseminated disease at diagnosis and are generally not curable. Patients can live a long time with indolent lymphomas because they tend to respond well to treatment and can remain in remission for many years or even decades. However, over time, some indolent lymphomas may transform into high grade lymphomas.
High grade lymphomas (aggressive lymphomas) grow and spread more quickly than low grade lymphomas. Destructive growth pattern of the deep lymph nodes within the chest or abdomen may press against various internal organs, causing difficult breathing, cough, poor appetite, weight loss, abdominal pain and distension, constipation, fever and legs swelling. Many patients with aggressive lymphomas can be cured by chemotherapy that kill rapidly dividing tumour cells.
Anyone who has an enlarged lymph node that does not return to normal size within few weeks and/or persistent symptoms should see a doctor immediately to make sure that lymphoma or another serious condition is not present.
How is the diagnosis made? An accurate pathologic diagnosis is the most important first step in the management of lymphomas. An incisional or excisional lymph node biopsy in combination with immunohistochemistry (IHC) is recommended to establish the diagnosis of lymphoma. IHC is essential for the differentiation of various subtypes. Fine needle aspiration (FNA) is inadequate for reliable diagnosis and grading. Other special test includes cytogenetic analysis, which involves examination of chromosomes from lymphoma cells under a microscope to check for any abnormalities in number or structure. The result of cytogenetic analysis often helps doctors to determine which type of lymphoma a patient has.
What is the workup for lymphoma? Essential workup procedures include: 1. Physical examination 2. Laboratory: blood count, lactate dehydrogenase, metabolic panels, hepatitis viruses, HIV 3. Bone marrow aspiration, trephine biopsy +/- immunophenotyping (for staging purpose). 4. Imaging: chest X-ray, CT neck, chest, abdomen, pelvis (for staging purpose) 5. Electrocardiograph (ECG) and echocardiogram 6. Optional: PET CT scan, lumbar puncture, brain MRI (depending on subtype & site)
What are the treatment options available? Treatment results for lymphomas have improved dramatically over the past four decades. The advent of more effective treatment options has improved the 5-year survival rates. Treatment for lymphoma varies widely based on the subtype. Treatment options include: 1. Watchful waiting (for low grade lymphomas) 2. Chemotherapy +/- immunotherapy (monoclonal antibody) 3. Radiotherapy 4. Stem cell transplantation (autologous, allogeneic) 5. Chimeric antigen receptor (CAR) T-cell therapy 6. Novel agents 7. Clinical trials
What is the prognosis? The prognosis is based on the stage at which the disease is diagnosed and determined by the lymphoma subtype, in addition to other factors such as performance status, age and other medical issues. Treatment for HL is highly effective and most patients are eventually cured. The survival rate for HL is generally higher than that of NHL. The American Cancer Society reports 5-year overall survival rate of 80% for HL and 72% for NHL. Various prognostic indices have been developed for different forms of lymphoma. The International Prognostic Index (IPI) was developed for aggressive NHL and validated in all clinical grades of NHL as a predictor of response to therapy, relapse and survival. The IPI is based on five factors: age, performance status, lactate dehydrogenase level, number of extra-nodal sites and stage of the disease.
Dr Teoh Ching Soon
Clinical Haematologist & Physician
MD (UPM), MRCP (UK), F’ship in Clinical Haematology (Malaysia), F’ship in Bone Marrow & Stem Cell Transplantation (Taiwan)
Dr Teoh Ching Soon is the Clinical Haematologist & Physician in Loh Guan Lye Specialists Centre. He has a keen interest in the management of malignant haematological disorders such as leukaemia, lymphoma, multiple myeloma, myelodysplastic syndrome and myeloproliferative neoplasm. His clinical work also focuses on benign haematological diseases, red cell and platelet disorders, coagulation and haemostasis, consultative haematology and haematopoeitic stem cell transplantation.
Your child hardly speaks like other children their age do. Does that automatically mean that your child has autism? Not necessarily. Even though speech delays and language delays often go hand in hand with autism, there are key differences between communication delays caused by autism and other types of speech-language disorders.
SPEECH DELAY VS LANGUAGE DELAY While speech and language delays are often confused and used interchangeably, there are distinguishing characteristics.
Speech delay: A disorder which affects ‘how’ children verbalise, articulate and control the sounds that are used in words. The children may be following typical speech patterns, but at a slower rate than their peers. Three major types of speech disorder include articulation, fluency, and voice disorders.
Language delay: A disorder which affects ‘what’ the children say. In other words, they are able to pronounce words well, but fail to form them effectively for others to understand. In addition, a receptive language delay can affect how children process information, be it verbal, nonverbal or written.
Autism is not the only cause to speech and language delays. Other causes, including hearing loss, deprivation of time talking with adults, bilingual environment, and etc. could also lead to the delays.
AUTISM Autism is also often called Autism Spectrum Disorder (ASD). It is a neurological and developmental disorder that causes significant social, communication and behavioural challenges. Children with ASD may have trouble understanding the world around them. Since autism is a spectrum disorder, the learning, thinking, and problem-solving abilities of children with ASD can range from highly skilled to severely challenged.
Concerning how ASD can be diagnosed, the leading medical reference is the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5). The core symptoms of autism are social communication challenges and restricted or repetitive behaviours. The severity of the symptoms varies among the affected children. Symptoms include avoidance of eye contact with people, not responding to name, not looking at objects when parents point. Children with ASD may not notice when other people around them appear sad or hurt. They show little interest, if any, to play with other children. Stimming, or repetitive unusual body movements or noises, is also one of the typical autistic children’s behaviours. They like to line up toys in a set order, or may get upset when there are minor changes. If parents notice any of these signs that worry them, it is advisable to seek medical attention.
Regardless of the complexity of ASD, following treatments can make a difference to the children and their families. i. Speech and language therapy aims to help children with ASD to communicate and interact better. ii. Occupational therapy provides assessment and intervention to maximise activities of daily living. iii. Applied behaviour analysis encourages desired behaviours and discourages undesired behaviours in children with ASD. iv. Parent education improves parent-child interaction and communication skills. v. Cognitive behaviour therapy helps children to cope with anxiety and depression.
THE EARLIER, THE BETTER Parents may spot the signs and symptoms at home, but they cannot diagnose the subject without an expert’s help. Early intervention programs are proven to be highly effective. If a child is not developing social and communication skills on par with the standards, do not hesitate to make an appointment with a professional. The journey of raising a child is tough enough, let alone a child with ASD, but who knows, you may find some extraordinary talent in them!
Dr Long Wai Lup
Paediatrician
MD (Russia), MRCPCH (UK)
Dr Long Wai Lup is a Paediatrician in Loh Guan Lye Specialists Centre. He attained his medical degree in 2009. His special care and interest towards childcare fuelled his desire to specialise in Paediatrics subsequently. He graduated from the Royal College of Paediatrics and Child Health UK (MRCPCH) in 2019. Dr Long has special interest in treating children with: • Developmental delay such as delay in speech-language development, motor skill and others • Skin illness in children including: Eczema, Infection, Allergy and others • Feeding issues from newborn to childhood • Growth issues in newborn to childhood
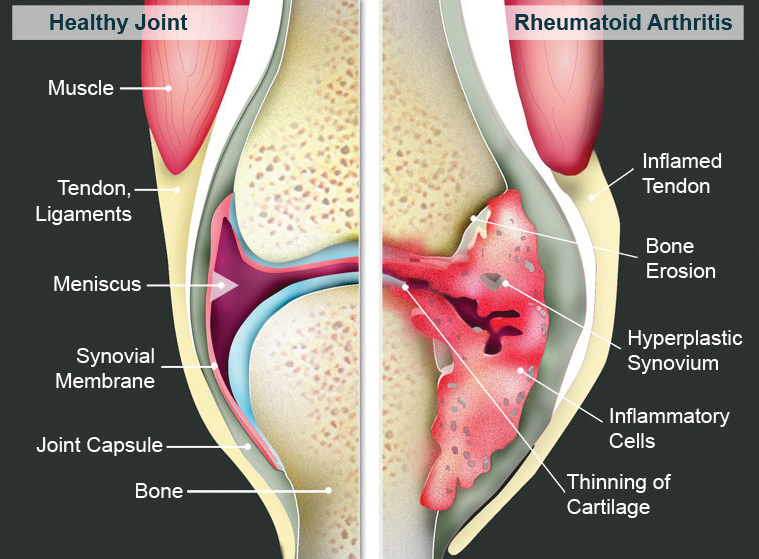
Rheumatoid arthritis (RA) is a type of chronic debilitating inflammatory arthritis that usually affects small joints of hands and feet. If not treated adequately, RA may cause severe pain and joint damage leading to permanent joint deformity.
How common is RA Worldwide, the prevalence of RA is estimated to be 0.24% of the population (Global Burden of Disease 2010 Study). In US and European countries, RA has a higher prevalence (0.5%- 1.0% of the population). In South-east Asia, the prevalence of RA was reported to be 0.40% (J Glob Health 2015). RA is found twice as common in women compared with men and more commonly found between 30-50 years old.
What causes RA RA is an autoimmune disease. To date, the exact cause of RA is not able to be identified. Researchers believe the occurrence of RA is multifactorial. A positive family history, genetic factor, smoking, obesity, physical inactivity, age and female sex have been reported to increase the risk of RA.
Presentations and symptoms of RA Commonly, RA patient will experience stiffness of hands/ feet or affected joints for more than an hour during early mornings. Joint pain and swelling are common. Joints involvement are usually symmetrical on both sides and joint distributions are polyarticular in nature. Apart from joint symptoms, patient may suffer from dry eye, dry mouth, lethargy, weight loss, nodules on skin, lung fibrosis or skin ulcer.
Diagnosis and investigations Diagnosis of RA is made based on patient’s history, physical examination, blood and imaging tests. Physical examination may reveal boggy joint swelling and joint tenderness on palpation. Patient may have deformities such as radial/ ulnar deviation of the wrist, wrist subluxation, ‘boutonniere deformity’ (hyperextension of the distal inter-phalangeal joint and flexion of the proximal inter-phalangeal joint), or ‘swan-neck’ deformity (hyperextension of the proximal inter-phalangeal joint and flexion of the distal inter-phalangeal joint).
Blood test for specific autoantibodies associated with RA are rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibody (ACPA). A positive RF or ACPA may indicate a more severe/ aggressive disease. Inflammatory markers such as erythrocyte sedimentation rate (ESR) or c-reactive protein (CRP) may be elevated in active disease.
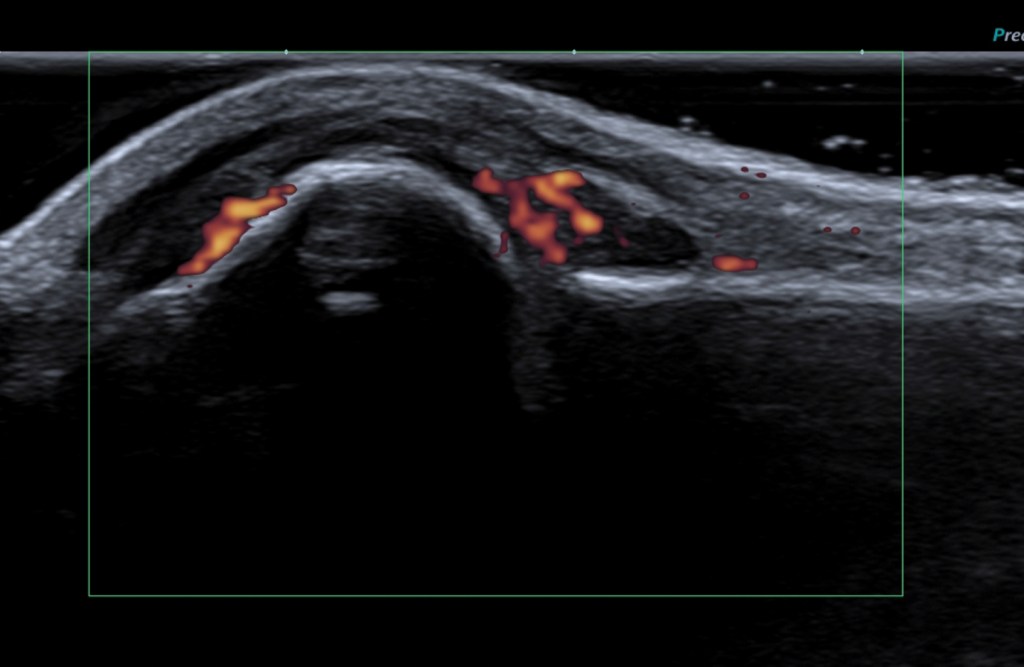
Imaging such as x-ray and ultrasonography of the affected joints may help to detect joint inflammation or erosion on the bones. Musculoskeletal ultrasound is widely used in rheumatology outpatient clinic as a diagnostic tool because ultrasound is more sensitive to detect early arthritis. Ultrasound is a non expensive, non-invasive safe procedure that does not use radiation when compared to other imaging modalities.
X-ray of the hands showed erosion at the carpal bones.Sonography of the left second metacarpo-phalangeal joint showed synovial hypertrophy and increase in power doppler signal that indicate active synovitis.
Differential diagnoses of RA Other than RA, the differential diagnoses of chronic inflammatory polyarthritis are: – – Gouty arthritis- polyarticular – Psoriatic arthropathy – Generalized erosive osteoarthritis – Arthritis related to connective tissue disease such as systemic lupus erythematosus (SLE)
Treatment Treatment of RA should be initiated as soon as the diagnosis of RA to preserve joint function and prevent joint deformity. The mainstay treatment of RA is disease modifying anti-rheumatic drugs (DMARDs). Example of commonly used conventional DMARDs are methotrexate, leflunomide, sulfasalazine and hydroxychloroquine. Biologic therapy or small molecule targeted therapy are also an option to treat severe RA whom have failed conventional DMARDs. Non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids may be used as an add-on therapy to reduce joint inflammation.
Non-pharmacological treatment is also important as part of RA treatment. Physiotherapy or occupational therapy may help in maintaining joint activity, strength and joint protection.
Complication of RA Untreated RA may cause severe disabling joint deformity. Apart from joint complication, RA may cause premature cardiovascular disease, lung fibrosis, osteopenia or osteoporosis, dry eyes and mouth, increased risk of cancer such as lymphoma.
What should I do if suspected to have RA If you have symptoms of arthritis, please consult your doctor. If investigations and further management are required, referral to Rheumatologist is warranted.
Dr Lim Chong Hong is a Consultant Rheumatologist & Physician in Loh Guan Lye Specialists Centre, Penang. He has vast experience in diagnosing and treating various rheumatic diseases/connective tissue diseases such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, gout, degenerative joint diseases and systemic lupus erythematosus (SLE).
by Chng Tian Ying, Head Sports Trainer – RMIT University
When it comes to the management and rehabilitation of soft tissue injuries, there is much complexity involved. What is a soft tissue injury? Soft tissue injuries commonly involve sudden trauma or overuse to muscles, ligaments, or tendons. These injuries often occur during sports and exercise activities but can also be sustained in a situation such as from a misstep when walking, and in many more different scenarios.
The most common traditional first aid protocols for soft tissue injuries were the mnemonics R.I.C.E. (Rest, Ice, Compression, Elevation), P.R.I.C.E. (Protection, Rest, Ice, Compression, Elevation) or P.O.L.I.C.E. (Protection, Optimal Loading, Ice, Compression, Elevation).
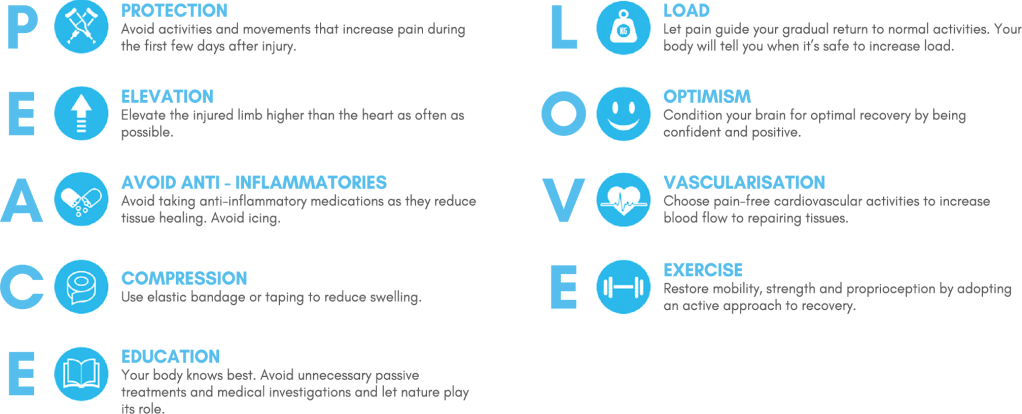
These methods highlight the acute management of soft tissue injuries but do not cover the sub-acute and chronic stages of these injuries. In 2019, Blaise Dubois and Jean-Francois Esculier proposed a new protocol: P.E.A.C.E and L.O.V.E.
The PEACE and LOVE protocol is a new comprehensive guide that covers all stages of injury. It also emphasises the importance of patient education and the biopsychosocial model.
Current research has shown that an individual’s experience of pain is influenced by the complex interactions between their biological, psychological, and social factors; Thus, it is essential that they receive equal attention to optimise the individual’s recovery process.
This protocol is split into two parts. PEACE is used as immediate care in the acute stage (1-3 days) after injury, and LOVE as ongoing management in the subsequent phases of injury.
In the past, movement and exercise after injury have been frowned upon because of the fear of re-injury, but recent research has suggested that introducing easy and gentle movement during the early stages of injury can be beneficial. It can help with blood flow, joint mobilisation, and decreased fear to get back into activity later. It has been suggested that movement is safe as long as it does not exceed a 4/10 pain, does not worsen the existing condition, and is not done excessively.
You may be wondering why ice has not been suggested in this protocol as one familiar scene that has been seen repeatedly, especially in the sporting community, is the use of ice during the early stages of a soft tissue injury.
The PEACE and LOVE protocol holds a controversial opinion towards the use of ice. Despite ice being widely used, there is no high-quality evidence to back up the efficacy of it. It has been suggested that although it can help relief pain, it could also potentially disrupt the inflammatory process and delay healing, as inflammation is the body’s natural response to heal and repair damaged tissue. The avoidance of anti-inflammatories is also suggested for a similar reason.
With the continual advancement of research comes new knowledge; therefore, leading to the constant evolvement of treatment and rehabilitation strategies. This article is a brief introduction to the PEACE and LOVE protocol, and more details can be found online.
With that being said, if you do experience a soft tissue injury in future, don’t forget to treat them with PEACE and LOVE!
by Dr Hayden Pooke, Chairman of the Sports Chiropractic Council Malaysia (SCCM)
The formation of Malaysia’s National Chiropractic Sports Council (NCSC), the Sports Chiropractic Council Malaysia (SCCM) was announced by the Association of Chiropractic Malaysia (ACM) at the beginning of 2020 and it was officially recognised by the International Federation of Sports Chiropractic (FICS) in 2021.
According to the SCCM Chairman and Sports Chiropractor, Dr Hayden Pooke, the SCCM’s membership increased from 13 to 47 members in 2021 and he hopes that the trend continues as the Malaysian Sporting Sector begins to open up and travel restrictions are reduced.
Before the Covid 19 national lockdown, the SCCM was involved in their first ever event in the Zurich PGAM Junior Invitational Tournament in 2020, invited by the Professional Golf Association of Malaysia.
Despite ongoing challenges from Covid-19, the SCCM is currently collaborating with Malaysian Sports Associations and plans to provide Sports Chiropractic care for athletes at as many events as possible in 2022.
SCCM is also poised to conduct, with FICS, their first International Certificate in Sports Chiropractic (ICSC) “hands-on” seminar in the third quarter of 2022 in Malaysia. The SCCM is also proud to announce that one of their student members Kong Hong Lian was awarded one of the FICS Student Scholarships for 2022, a first for any Malaysian Chiropractic Student.
Apart from producing world class Sports Chiropractors by completing the FICS highly acclaimed ICSC and giving its members the opportunity to represent FICS Sports Chiropractic delegations at international sports events treating world class athletes, SCCM also pledges to do everything it takes to bring Sports Chiropractic treatment to the local Malaysian sporting scene, servicing and educating athletes at all levels of competition.
I believe some of us have come across stem cells treatment in certain diseases. In orthopaedic, stem cells have been used to treat osteoarthritis, for example knee osteoarthritis, etc. Much has been said and heard about stem cells treatment but I believe the knowledge of the general population on stem cells treatment is still superficial. Thus, it is better for everyone to learn a little more about it.
Stem cells are undifferentiated cells with the ability and potential to self-renew and proliferate, producing more differentiated or specialised cells in the process. Stem cells can be obtained from several sources; they have several types, namely embryonic stem cells, perinatal stem cells, induced pluripotent stem cells, adult stem cells(Mesenchymal, hematopoietic and epithelial) and immune stem cells.
With the advancement and research development of stem cells technology, stem cells therapy has been able to expand its therapeutic function. Stem cells have been used as a cell source to reconstruct or rebuild living tissue. In the field of immunotherapy, stem cells have been used as an immune modulator for autoimmune diseases. Furthermore, it can also act as progenitor cells for immunotherapy, allowing the development of cellular technology for anti-cancer, anti-virus and enhancement of body immune system. Because of its potential to self-renew and proliferate, stem cells is also used as a therapeutic agent for degenerative diseases related to aging and frailty, and it has been developed into drugs for treatment of chronic and resilient illnesses. With recent advancements, stem cells therapy has been introduced into the treatment of autism and it has shown promising results.
After several decades and continuous research, stem cells therapy will become a game changer for the future in medicine. The capabilities of stem cells are growing everyday although there are still many obstacles to overcome. It is undeniable that stem cells play a huge role in regenerative medicine and transplantology, but because the technology that produces stem cells is expensive, only few could afford it. With the establishment of more regulated stem cells laboratories, I believe stem cells therapy could be more affordable to everyone that requires it.
by Dr Tan Kenny – Consultant Neurologist & Physician
(Subspecialty in Parkinson’s Disease & Movement Disorders)
Having sudden facial or limb weakness and numbness? Sudden slurred speech or drooling? Sudden blurred vision? Is that a concern? What is going on with your body?
Stroke is preventable and treatable. It is important to recognise early stroke symptoms and BE FAST to act during the golden hour so that immediate emergency stroke treatment can be initiated to reduce brain injury.
Stroke occurs when there is reduced blood supply to the brain. In general, stroke can be classified based on the etiology of reduced blood supply, i.e. ischemic (blockage) and hemorrhagic (bleed). Ischemic stroke is the most common type of stroke. Symptoms suggestive of stroke include sudden poor balance, visual problems, face or limb weakness or numbness, speech difficulty. An easy acronym to remember is BE FAST (Balance Difficulties, Eyesight Changes, Face Weakness, Arm Weakness, Speech Difficulties, Time to call for help).
Around 2 million brain cells die every minute during acute stroke, increasing the risk of permanent brain damage, disability or death. Thus, it is pertinent to identify stroke early so that the necessary medical treatment can be implemented.
Upon reaching the hospital, the neurologist will initiate emergency stroke assessment to establish the diagnosis of ischemic stroke before initiating acute stroke treatment. One such treatment is thrombolytic therapy, i.e., administration of a ‘clot buster’ medication to dissolve blood clots that have blocked the arteries in the brain causing stroke, in the hopes of breaking the clot to reperfuse and return blood flow to the affected brain cells. To be effective, the therapy needs to be initiated as soon as possible within the golden hour (4.5 hours from the onset of symptoms), before permanent irreversible damage has occurred.
For ischemic stroke patients who arrive beyond the treatment window period (>4.5 hours) and not suitable for acute thrombolytic therapy, appropriate investigations and medical treatment to stabilise patient will be initiated i.e. blood thinners, blood pressure and blood sugar control. The first three months after a stroke are the most important for recovery as patients will see the most improvement. Thus, besides providing best medical treatment, patient will require neuro-rehabilitation i.e. physiotherapy, occupational therapy and speech therapy.
Stroke can be debilitating but the bright side is it can be prevented and may be attributed to modifiable and non-modifiable risk factors
In Malaysia, hypertension was the most common risk factor followed by diabetes mellitus. Modifiable risk factors are the focus of primary prevention and they include the following risk factors:
a) Lifestyle, i.e., smoking, unhealthy diet, lack of physical activity.
b) Metabolic, i.e., hypertension, diabetes, high cholesterol, obesity (measured by high body mass index or BMI)
c) Environmental, i.e., stress, air pollution.
Many are not aware that stroke can recur. The recurrence rates are 3-4% in the first month and 12% in the first year after a stroke. This emphasises the importance of secondary stroke prevention, and this may involve medical interventions including anti-platelet therapy, anti-hypertensive treatment, cholesterol and blood sugar control. Besides compliance to medication, lifestyle modification plays a vital role.
It is recommended to maintain an active lifestyle by exercising 30 mins daily or at least 150 mins per week, stop smoking, avoid heavy alcohol drinking and healthy diet. Mediterranean diet (low glycemic with high intake of vegetables) supplemented with nuts, diet high in fruits and leafy green vegetables are beneficial. It is also recommended to follow the Dietary Approaches to Stop Hypertension (DASH diet) to reduce blood pressure, emphasising on high consumption of fruits, vegetables, whole grains, low-fat dairy foods, legumes and nuts, and low intake of sodium, sweetened beverages, and red and processed meat.
In Malaysia, there is still lack of awareness in regards to recognition of stroke symptoms and the significance of time-sensitive stroke treatment. As a result, delay in early intervention may lead to prolonged hospital stay and increase of stroke-related morbidities and mortality. BE FAST to ensure better outcome as time loss is brain loss in acute stroke. Stroke strikes fast, so should you.
Dr Tan Kenny is a Consultant Neurologist and Physician at LohGuanLye Specialists Centre. He has vast experience in diagnosing and managing stroke, dementia, headaches, Parkinson’s and various other neurological conditions. He established the emergency neurology stroke service at LohGuanLye Specialists Centre and obtained the World Stroke Organization (WSO) Angels Award Platinum Status for the hospital’s stroke service. He is committed to creating awareness, education and holds the position as the Medical Advisor for the Penang Parkinson’s and Rehabilitation Association.
How a series of sleep loss impacts mental & physical wellbeing Three consecutive nights of sleep loss can have a negative impact on our mental and physical health and cause both to greatly deteriorate. Sleep deprivation can lead to an increase in anger, frustration, anxiety and a weakened immune system and amongst others.
A new study published in Annals of Behavioural Science looked at the consequences of sleeping fewer than six hours for eight consecutive nights – six hours is the minimum duration of sleep that experts say is necessary to support optimal health in average adults.
Lead author Soomi Lee, Assistant Professor in the School of Aging Studies at the University of South Florida, found the biggest jump in symptoms appeared after just one night of sleep loss. In a study by the University, the number of mental of physical problems steadily got worse, peaking on day three. At that point, the research showed that the human body has gotten relatively used to repeated sleep loss. But all that changed on day six, when participants reported that the severity of physical symptoms was at its worst.
Many of us think that we can pay back our ‘sleep debt’ on weekends and be more productive during the week. However, results from this study shows that having just one night of sleep loss can significantly impair your daily mental abilities and functioning.
Data provided by the Midlife, included a study of nearly 2,000 middle-aged adults who were relatively healthy and well-educated. Among them, 42 percent had at least one night of sleep loss, sleeping one and a half hours than typical routines.
They recorded their mental and physical behaviours in a journal for eight consecutive days, allowing researchers to review, how SLEEP LOSS causes wear and tear on the body.
Participants reported a pile-up of angry, nervous, lonely, irritable and frustrated feelings as a result of sleep loss. They also experienced more physical symptoms, such as upper respiratory issues, aches and pain, gastrointestinal problems, and other health concerns.
These negative feelings and symptoms were continuously elevated throughout consecutive sleep loss days and did not return to baseline levels unless they had a night’s sleep of more than six hours.
About one third of adults sleep less than six hours per night. Once that becomes a habit, it’s increasingly difficult for your body to fully recover from lack of sleep, continuing the vicious cycle of worsening daily wellbeing, which could impact one professionally.
A previous study led by author Sommi found losing just 16 minutes of sleep could impact job performance. Her previous findings also showed that minor sleep loss can decrease daily mindfulness, which is a critical recourse for managing stress and maintaining healthy routines.
So, I would advise the best way to maintain a strong daily performance is to set aside more than SIX HOURS of SLEEP NIGHTLY.