

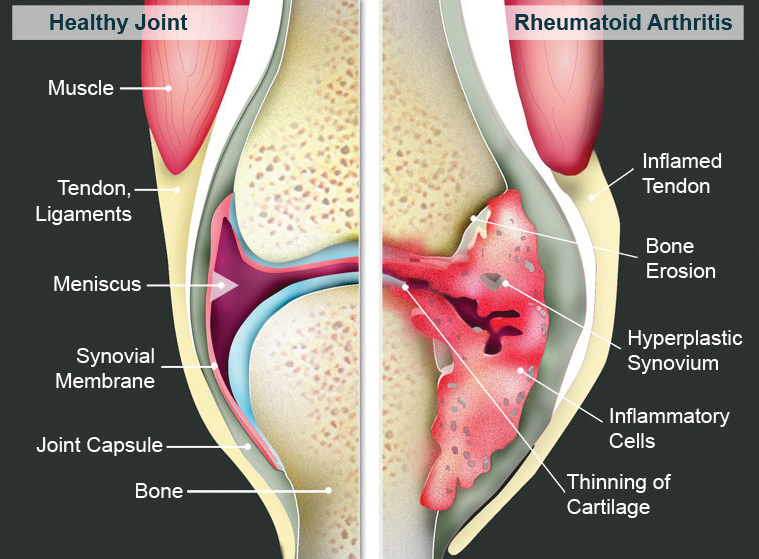
Rheumatoid arthritis (RA) is a type of chronic debilitating inflammatory arthritis that usually affects small joints of hands and feet. If not treated adequately, RA may cause severe pain and joint damage leading to permanent joint deformity.
How common is RA
Worldwide, the prevalence of RA is estimated to be 0.24% of the population (Global Burden of Disease 2010 Study). In US and European countries, RA has a higher prevalence (0.5%- 1.0% of the population). In South-east Asia, the prevalence of RA was reported to be 0.40% (J Glob Health 2015). RA is found twice as common in women compared with men and more commonly found between 30-50 years old.
What causes RA
RA is an autoimmune disease. To date, the exact cause of RA is not able to be identified. Researchers believe the occurrence of RA is multifactorial. A positive family history, genetic factor, smoking, obesity, physical inactivity, age and female sex have been reported to increase the risk of RA.
Presentations and symptoms of RA
Commonly, RA patient will experience stiffness of hands/ feet or affected joints for more than an hour during early mornings. Joint pain and swelling are common. Joints involvement are usually symmetrical on both sides and joint distributions are polyarticular in nature. Apart from joint symptoms, patient may suffer from dry eye, dry mouth, lethargy, weight loss, nodules on skin, lung fibrosis or skin ulcer.
Diagnosis and investigations
Diagnosis of RA is made based on patient’s history, physical examination, blood and imaging tests. Physical examination may reveal boggy joint swelling and joint tenderness on palpation. Patient may have deformities such as radial/ ulnar deviation of the wrist, wrist subluxation, ‘boutonniere deformity’ (hyperextension of the distal inter-phalangeal joint and flexion of the proximal inter-phalangeal joint), or ‘swan-neck’ deformity (hyperextension of the proximal inter-phalangeal joint and flexion of the distal inter-phalangeal joint).
Blood test for specific autoantibodies associated with RA are rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibody (ACPA). A positive RF or ACPA may indicate a more severe/ aggressive disease. Inflammatory markers such as erythrocyte sedimentation rate (ESR) or c-reactive protein (CRP) may be elevated in active disease.
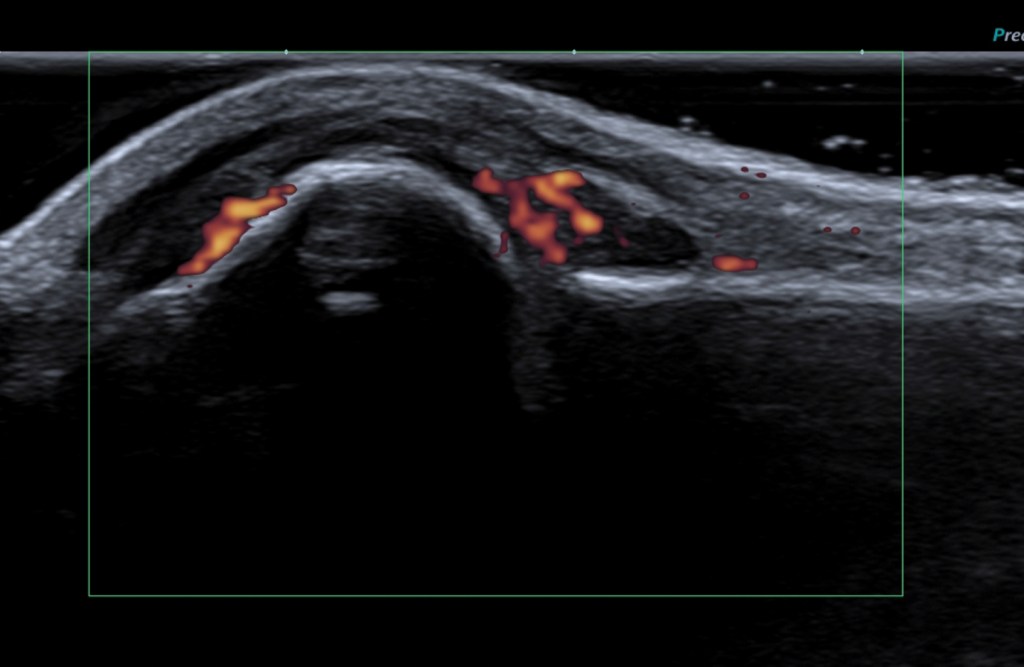
Imaging such as x-ray and ultrasonography of the affected joints may help to detect joint inflammation or erosion on the bones. Musculoskeletal ultrasound is widely used in rheumatology outpatient clinic as a diagnostic tool because ultrasound is more sensitive to detect early arthritis. Ultrasound is a non expensive, non-invasive safe procedure that does not use radiation when compared to other imaging modalities.

Differential diagnoses of RA
Other than RA, the differential diagnoses of chronic inflammatory polyarthritis are: –
– Gouty arthritis- polyarticular
– Psoriatic arthropathy
– Generalized erosive osteoarthritis
– Arthritis related to connective tissue disease such as systemic lupus erythematosus (SLE)
Treatment
Treatment of RA should be initiated as soon as the diagnosis of RA to preserve joint function and prevent joint deformity. The mainstay treatment of RA is disease modifying anti-rheumatic drugs (DMARDs). Example of commonly used conventional DMARDs are methotrexate, leflunomide, sulfasalazine and hydroxychloroquine. Biologic therapy or small molecule targeted therapy are also an option to treat severe RA whom have failed conventional DMARDs. Non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids may be used as an add-on therapy to reduce joint inflammation.
Non-pharmacological treatment is also important as part of RA treatment. Physiotherapy or occupational therapy may help in maintaining joint activity, strength and joint protection.
Complication of RA
Untreated RA may cause severe disabling joint deformity. Apart from joint complication, RA may cause premature cardiovascular disease, lung fibrosis, osteopenia or osteoporosis, dry eyes and mouth, increased risk of cancer such as lymphoma.
What should I do if suspected to have RA
If you have symptoms of arthritis, please consult your doctor. If investigations and further management are required, referral to Rheumatologist is warranted.
Dr Lim Chong Hong
Consultant Rheumatologist & Physician
MD (UPM), MRCP (UK), FRCP (Edin.), Fellowship in Rheumatology (Mal & Taiwan), CMIA (NIOSH)
Dr Lim Chong Hong is a Consultant Rheumatologist & Physician in Loh Guan Lye Specialists Centre, Penang. He has vast experience in diagnosing and treating various rheumatic diseases/connective tissue diseases such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, gout, degenerative joint diseases and systemic lupus erythematosus (SLE).
