by Dr. Lim Shyang Yee,
General, Upper Gastrointestinal & Bariatric Surgeon
Gastro-esophagus junction is where your food pipe (esophagus) joins the stomach. Cancer which starts from the inner lining of this junction is called gastro-esophagus cancer.
It may be sometimes difficult to tell the difference between stomach, esophagus and gastro-esophagus cancer. In combination esophagus and stomach cancer are the 4th most common cancer. Both cancers in combination are the second most cause of cancer deaths in Malaysia. They can behave differently to cancers of the stomach and esophagus.
In Malaysia, the incidence of esophagus cancer located at the gastro-esophagus junction has increased from 55% to nearly 70% over the last 15 years. Yet 70-80% of patients with this cancer present to specialist very late either stage III or IV of the disease.
Who is at risk?
• Chronic Gastroesophagus Reflux Disease (with or without Hiatus Hernia)
• Obesity: Higher incidence of hiatus hernia and GERD
• Barrett’s Esophagus: Pre-cancerous condition.
• Smoking & Excessive Alcohol
How do I know?
Early cancer does not have a specific symptom. Dyspepsia or indigestion is a non-specific symptom. Most patients have difficulty of swallowing by the time they seek consultation.
Upper endoscopy examination under sedation (inserting a flexible camera inside the esophagus and stomach through the mouth) to visualize any growth and take sample for confirmation of the diagnosis.
Once diagnosis is confirmed, radiology imaging like PET-CT scan to determine the stage of the cancer and doctor to discuss treatment option.
Can this cancer be cured?
Stage of cancer determined the curability of the cancer. If pre-cancerous condition like Barrett’s esophagus is detected early on endoscopy, it can be burned with endoscopic radiofrequency ablation (RFA) and prevent progression to cancer.
Early cancer can be treated with endoscopic resection (shaving the inner layer of the gastro-esophagus mucosa/lining).
Advanced stage II and III cancer require pre-operative treatment of chemotherapy before surgical removal of the lower end of esophagus and removal of affected the lymph nodes. If the cancer has spread to significant portion of the stomach, the stomach will require complete removal.
Can I still able to eat after stomach or esophagus resection?
After surgical removal of the disease esophagus and small portion of the stomach, the remaining stomach will be used to restore the continuity of the food passage. After recovering from surgery, food must be properly chewed for smooth swallowing.
For cancer that spreads to the stomach and require total removal of the stomach, the small or large intestine (colon) will be used to restore the continuity of the food passage. After recovering from surgery, patient will still be able to eat and consume smaller portion of food with proper chewing and frequent meals. As absorption of food nutrient occur in the small intestine, most patient can live with their regular food and vitamin B12 supplements.
How is the recovery after surgery?
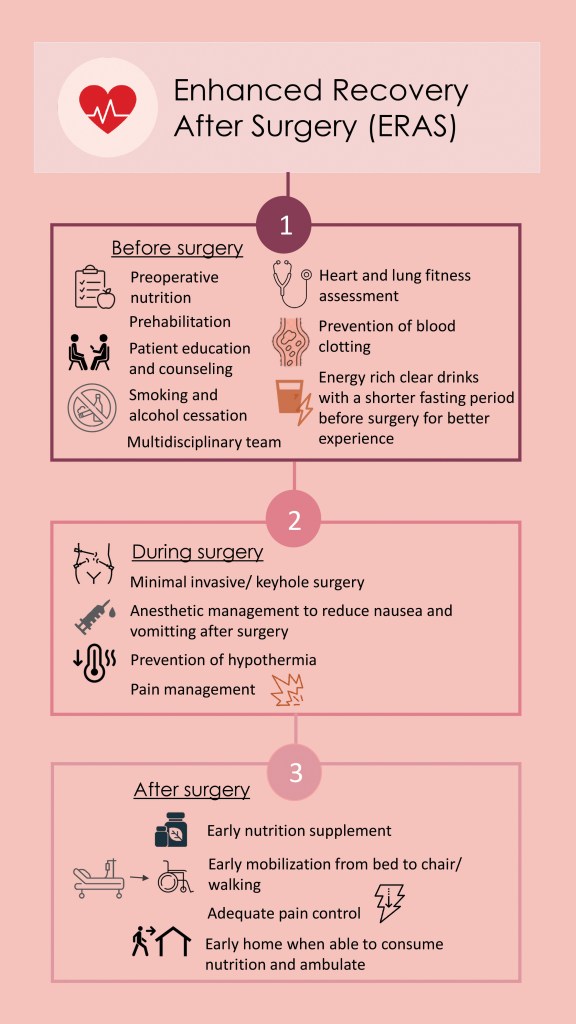
Surgery to remove the gastro-esophagus cancer is a major complex surgery. Enhanced recovery after surgery (ERAS) pathway is beneficial for patient who undergoes major complex surgery. Before going for a major sport event athletes undergo proper physical training and adequate preparation & nutrition. Likewise this surgery needs pre-habilitation (activity to improve functional capability and enhanced general wellness before surgery) with adequate pre-surgery nutrition supplements, stop smoking and stabilizing the patient’s co-existing medical conditions before embarking on surgery.
Minimal invasive surgery (keyhole or laparoscopic surgery) can be performed with less post-operative pain and early ambulation.
Is gastro-esophagus cancer preventable?
Maintaining a healthy weight, early treatment of GERD and pre-cancerous Barrett’s esophagus can prevent this cancer. Early upper endoscopy is essential for early detection and better survival.